Review of transcranial photobiomodulation for major depressive disorder: targeting brain metabolism, inflammation, oxidative stress, and neurogenesis
Paolo Cassano; Samuel R. Petrie; Michael R. Hamblin; Theodore A. Henderson; Dan V. Iosifescu; - Neurophotonics, 3(3), 031404 (2016). doi:10.1117/1.NPh.3.3.031404 March 4, 2016 (Publication) 4471 This study shows some of the most detailed parameters (power, wavelenght, dosage) for working with the brain and seems to be unbiased because of the diverse background of authors..
We examined the use of near-infrared and red radiation (photobiomodulation, PBM) for treating major depressive disorder (MDD). While still experimental, preliminary data on the use of PBM for brain disorders are promising. PBM is low-cost with potential for wide dissemination; further research on PBM is sorely needed. We found clinical and preclinical studies via PubMed search (2015), using the following keywords: “near-infrared radiation,” “NIR,” “low-level light therapy,” “low-level laser therapy,” or “LLLT” plus “depression.” We chose clinically focused studies and excluded studies involving near-infrared spectroscopy. In addition, we used PubMed to find articles that examine the link between PBM and relevant biological processes including metabolism, inflammation, oxidative stress, and neurogenesis. Studies suggest the processes aforementioned are potentially effective targets for PBM to treat depression. There is also clinical preliminary evidence suggesting the efficacy of PBM in treating MDD, and comorbid anxiety disorders, suicidal ideation, and traumatic brain injury. Based on the data collected to date, PBM appears to be a promising treatment for depression that is safe and well-tolerated. However, large randomized controlled trials are still needed to establish the safety and effectiveness of this new treatment for MDD.
1.
Introduction
Infrared (IR) light is ubiquitously present to most life on the earth. Of the total amount of solar energy reaching the human skin, 54% is IR and 30% is IR type A—near-infrared—(NIR; with a wavelength range of 760 to 1440 nm),1 which penetrates through the human skin and reaches deeply into tissue, depending on wavelength and energy.2
NIR is used to treat a variety of conditions such as muscle pain,3 wounds,4 neuropathic pain,5 and headache.6 NIR is also used for wellness and lifestyle purposes such as for cosmetic improvement in peri-orbital wrinkles.7,8 The clinical use of NIR light applied in NIR-spectroscopy dates from the mid-1980s, when it was used for monitoring of the brain in the neonate and the fetus.9
The use of transcranial phototherapy for treating brain disorders started with its application to acute stroke. Numerous preclinical animal studies1011.–12 suggested that the application of NIR laser (810 nm) to the head at various times (hours) after induction of an acute stroke had beneficial effects on subsequent neurological performance and reduced lesion size. Evidence was obtained for the anti-inflammatory, anti-apoptotic, and proneurogenesis effects in the brain stimulated by this approach.13,14 These promising animal studies led to the conduction of a series of clinical trials called NeuroThera Effectiveness and Safety Trials (NEST). All together there were three large studies conducted in 1410 stroke patients [NEST-1 (n=120" role="presentation">n=120
)] that demonstrated that NIR light delivered transcranially with a class-IV laser is safe, with no significant differences in rates of adverse events with NIR, when compared to sham exposure.1516.–17 Other preclinical studies and clinical trials have suggested that transcranial photobiomodulation (PBM: laser or light emitting diodes—LED) is safe and effective for acute1819.20.21.–22 and chronic2324.–25 traumatic brain injury (TBI) and has beneficial effects on neurodegenerative diseases (Alzheimer’s and Parkinson’s).26,27
For the transcranial treatment of major depressive disorder (MDD), both PBM LEDs and lasers have been experimentally tested, although PBM is not FDA-approved for the treatment of MDD. Certain forms of PBM treatment are also referred to as low-level light therapy (LLLT), since it utilizes light at a low power (0.1 to 0.5 W output at the source) to avoid any heating of tissue. The irradiance of the PBM medical devices (or power density) typically ranges from 1 to 10 times the NIR irradiance from sunlight on the skin (33.6mW/cm2" role="presentation">33.6mW/cm2
at the zenith). However, most PBM medical devices only deliver light energy at one or two selected wavelengths, as opposed to the whole spectrum of IR that is contained in sunlight. To our knowledge and to this date, transcranial PBM treatment has not caused any retinal injury—one of the most likely postulated adverse events, although care is taken routinely in such studies to protect the eyes with goggles or eye covers.28
In this review, we will first discuss the mechanisms of action by which NIR and red light (PBM) might improve symptoms of depression, and then present the clinical evidence for their use as a treatment for MDD and other comorbid psychiatric syndromes.
2.
Methods
We found clinical and preclinical studies via PubMed search (December 15, 2015), using the following keywords: “near-infrared radiation,” “NIR,” “low-level light therapy,” “low-level laser therapy,” or “LLLT” plus “depression.” We chose studies that had a clinical focus, and we excluded studies involving NIR spectroscopy. We also located studies using the references from the articles found in the PubMed search. As the searched literature encompassed different conditions and disorders frequently comorbid with depression, a specific section of this review was devoted to the effect of PBM on psychiatric comorbidity. In the latter section, the following conditions were included, based on available literature: TBI, anxiety and post-traumatic stress syndromes, insomnia, and suicidal ideation. The literature search for the use of PBM to treat comorbid conditions was neither systematic nor extensive, but rather a secondary focus of this review. The information is presented in an organized fashion to allow the reader to easily grasp the potential applications of PBM for the treatment of depression and of its comorbid conditions. To attain this goal, the authors have allowed a margin of redundancy, by distributing different information derived from any given publication in separate sections of this review. To avoid an artificial inflation of the extant literature on the chosen topic, we referenced the main authors—and when appropriate their affiliation—when referring to the same articles more than once. The reader will find a table summarizing the six key clinical articles reviewed, also to avoid unintended inflation of the literature. The six clinical reports included in this review where extracted from a pool of 58 articles, that were originally identified with the literature search.
In addition, we used PubMed to find articles that examined the link between PBM and each of the various biological processes including metabolism, inflammation, oxidative stress, and neurogenesis.
3.
Targeting Brain Metabolism
Multiple studies have reported regional and global hypometabolism in MDD, which could be related (either causally or consequentially) to the neurobiology of mood disorders.2930.31.–32 Positron emission tomography studies have shown abnormalities in glucose consumption rates and in blood flow in several brain regions of subjects with major depression.33 Moreover, metabolic abnormalities in the anterior cingulate, the amygdala-hippocampus complex, the dorsolateral prefrontal cortex (DLPFC), and inferior parietal cortex seem to improve after antidepressant treatment or after recovery.3435.–36
With phosphorus magnetic resonance spectroscopy (P31-MRS" role="presentation">31P-MRS
), the baseline pool of nucleotide triphosphate (NTP)—a product of the cellular utilization of glucose and a marker of the cellular energy availability—was low in subjects who subsequently responded to antidepressant treatment.32 Iosifescu et al.32 also demonstrated for the first time with P31-MRS" role="presentation">31P-MRS a correlation between treatment response (to a regimen that combined antidepressants and triiodothyronine) and restoration of a higher NTP pool (with compensatory decrease in phosphocreatine) in the anterior cingulate cortex. This study suggests a pathway to antidepressant response based on restoration of a high cellular energy state. In fact, phosphocreatine represents a long-term storage depot of energy, while NTP and ATP are energy-rich molecules that are readily available to the cell. The same authors replicated the aforementioned findings in MDD subjects treated with standard antidepressants (Iosifescu et al., unpublished). In this cohort, P31-MRS" role="presentation">31P-MRS
metabolite changes were noted in brain-only voxels of responders, but not in nonresponders to antidepressants.
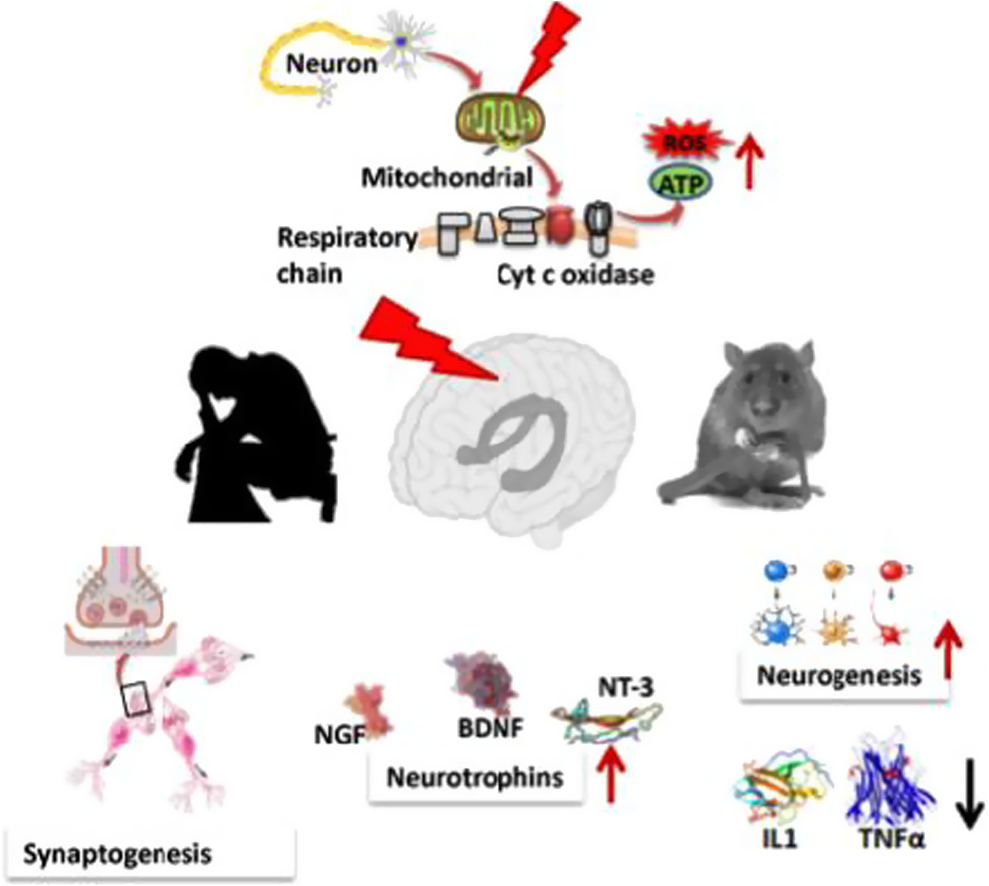
In experimental and animal models, PBM (NIR and red light) noninvasively delivers energy to the cytochrome c oxidase and by stimulating the mitochondrial respiratory chain leads to increased ATP production (see Fig. 1).3738.–39 A study of the effects of NIR on patients with MDD found that a single session of NIR led to a marginally significant increase in regional cerebral blood flow.40 Whether the observed changes in cerebral blood flow resulted from fundamental changes in neuronal metabolism or changes in vascular tone remain to be clarified. Given the correlation of both hypometabolism and abnormal cerebral blood flow with MDD, the beneficial effect of NIR on brain metabolism is one potential mechanism for its antidepressant effect.
Fig. 1
Cellular targets of NIR radiation mechanisms of transcranial NIR for psychiatric disease. The NIR photons are absorbed by cytochrome c oxidase in the mitochondrial respiratory chain. This mitochondrial stimulation increases production of ATP but also activates signaling pathways by a brief burst of ROS. This signaling activates antioxidant defenses reducing overall oxidative stress. Proinflammatory cytokines and neuroinflammation are reduced. Neurotrophins such as brain-derived neurotrophic factor are upregulated, which in turn activate synaptogenesis (formation of new connections between existing neurons) and neurogenesis (formation of new neurons from neural stem cells).
4.
Targeting Inflammation
Animal and clinical research suggests that the inflammatory arm of the immune system contributes to MDD. Post-mortem gene expression profiling on tissue samples from Brodmann area 10 (BA10—prefrontal cortex) have shown that MDD is characterized by increased inflammation and apoptosis.41 In a case-control study, Simon et al.42 found that antidepressant-naive MDD subjects had significant elevations in the following cytokines and chemokines when compared to healthy controls: MIP-1α" role="presentation">MIP-1α
. Although IL-10 is an anti-inflammatory cytokine, the results suggested that the elevated levels of this IL-10 were likely induced in response to the overall elevation of proinflammatory cytokine levels. In a review of the research on inflammation in MDD, Raison et al.43 proposed that proinflammatory cytokines might cause brain abnormalities that are characteristic of MDD. Indeed, animal research has shown that IL-1 mediates chronic depression in mice by suppressing hippocampal neurogenesis.44
One proinflammatory cytokine that may be of particular relevance to depression is CSF IL-6 (IL6 measured in cerebrospinal fluid). In a recent report, patients with MDD had significantly higher CSF IL-6 levels compared to healthy controls; CSF IL-6 levels were significantly higher than in the serum, and there was no significant correlation between CSF and serum IL-6 levels.45 These findings are consistent with a prior report showing a positive correlation between CSF IL-6 levels and the severity of depression and suicide attempts, with the strongest correlation found in violent suicide attempters.46 One report in a smaller sample of depressed patients has shown that CSF IL-647 was lower or comparable to healthy controls.
NIR light and red light (600 to 1600 nm) decreased synovial IL-6 gene expression (decreased mRNA levels) in a rat model of rheumatoid arthritis.48 In another study, NIR (810 nm) used as a treatment for pain in patients with rheumatoid arthritis decreased production of the following proinflammatory cytokines: TNF-α" role="presentation">TNF-α
, IL-1β" role="presentation">IL-1β
, and IL-8.49 Khuman et al.50 showed that transcranial NIR improved cognitive function and reduced neuroinflammation as measured by Iba1+ activated microglia in brain sections from mice that had suffered a TBI. Finally, NIR (970 nm) has been found to be an effective treatment for inflammatory-type acne.51 In summary, it is reasonable to predict that transcranial NIR treatment would likewise have an anti-inflammatory effect in patients suffering from MDD.
5.
Targeting Oxidative Stress
Research has demonstrated a correlation between MDD and vulnerability to oxidative stress.52 For example, depression-induced rats show a significant decrease in glutathione peroxidase (GSH-Px) activity in the cortex.53 Glutathione (GSH) is the most abundant and one of the important antioxidants in the brain; GSH-Px enzymes protect against oxidative stress via reducing hydroperoxides and scavenging free radicals.54 GSH also appears reduced in the brains of MDD subjects.55 Additionally, a study by Sarandol et al.52 demonstrated that MDD patients have higher levels of malondialdehyde, a toxic molecule and a biomarker of oxidative stress.56 Moreover, depressed patients have more red blood cell (RBC) oxidation compared to healthy controls.52 In the same study, the authors found a significant positive correlation between RBC superoxide dismutase (SOD) activity and depression severity. SOD serves to catalyze the removal of the toxic superoxide radical.57 Thus, elevated SOD activity in depressed patients might indicate higher levels of oxidative stress. Finally, catalase activity and nitric oxide (NO) levels have also been shown to be lower in depressed patients than in healthy controls.58 Catalase is an enzyme that protects cells against damaging reactive oxygen species (ROS) via degradation of hydrogen peroxide to water and oxygen.59 NO has protective effects against cell damage, which are likely due to its pleiotropic functions in regulating antioxidant enzymes and many other aspects of cell metabolism.60,61
Oxidative stress may be an effective target for antidepressant treatments. However, successful treatments for MDD vary in regard to their protective effects against oxidative stress.52,53,62 Animal research suggests that PBM may have beneficial effects on oxidative stress. In a rat model of traumatized muscle, NIR (904 nm) blocked the release of harmful ROS and the activation of the transcription factor, nuclear factor κB (NF-κB), both induced by muscle trauma. Trauma activates NF-κB by destroying a specific protein inhibitor of NF-κB called IκB, and this destruction was inhibited by NIR light. Furthermore, NIR reduced the associated overexpression of the inducible form of nitric oxide synthase (iNOS) and reduced the production of collagen.63 This regulation of iNOS is important because excessive levels of iNOS can lead to formation of large amounts of NO that combine with superoxide radicals to form the damaging species peroxynitrite, and can interfere with the protective benefits of other forms of NO synthase.64 These findings suggest that NIR protects against oxidative stress induced by trauma. Finally, an in vitro study of the effects of red light and NIR (700 to 2000 nm) on human RBCs found that NIR significantly protected RBCs against oxidation.65
Photobiomodulation for Traumatic Brain Injury and Stroke
Michael R Hamblin - J Neurosci Res. Author manuscript; available in PMC 2018 Oct 1. (Publication) 4533 This study compare wavelength and pulsing frequencies to find the highest efficacy. It shows how much better 810nm (fig 3)and 10Hz (fig 4) are superior for TBI.
There is a notable lack of therapeutic alternatives for what is fast becoming a global epidemic of traumatic brain injury (TBI). Photobiomodulation (PBM) employs red or near-infrared (NIR) light (600-1100nm) to stimulate healing, protect tissue from dying, increase mitochondrial function, improve blood flow and tissue oxygenation. PBM can also act to reduce swelling, increase antioxidants, decrease inflammation, protect against apoptosis, and modulate microglial activation state. All these mechanisms of action strongly suggest that PBM delivered to the head should be beneficial in cases of both acute and chronic TBI. Most reports have used NIR light either from lasers or from light-emitting diodes (LEDs). Many studies in small animal models of acute TBI have found positive effects on neurological function, learning and memory, and reduced inflammation and cell death, in the brain. There is evidence that PBM can help the brain to repair itself by stimulating neurogenesis, upregulating BDNF synthesis, and encouraging synaptogenesis. In healthy human volunteers (including students and healthy elderly women) PBM has been shown to increase regional cerebral blood flow, tissue oxygenation and improve memory, mood and cognitive function. Clinical studies have been conducted in patients suffering from the chronic effects of TBI. There have been reports of improvements in executive function, working memory, and improved sleep. Functional magnetic resonance imaging has shown modulation of activation in intrinsic brain networks likely to be damaged in TBI (default mode network and salience network).
Photobiomodulation (PBM) formerly known as low-level laser (light) therapy (LLLT) is approaching its 50th anniversary, after being discovered by Endre Mester working in Hungary in 1967 (Hamblin et al. 2016). Originally thought to be a property of red lasers (600-700 nm), PBM has broadened to include near-infrared (NIR) wavelengths 760-1200 nm, and even blue and green wavelengths. Moreover the advent of inexpensive and safe light emitting diodes (LEDs) has supplanted the use of expensive lasers in many indications. The better tissue penetration properties of NIR light, together with its good efficacy, has made it the most popular wavelength range overall. The best-known medical applications of PBM have been for indications such as stimulation of wound healing (Hopkins et al. 2004; Kovacs et al. 1974), reduction of pain and inflammation in orthopedic and musculoskeletal conditions (Aimbire et al. 2006; Gam et al. 1993), and mitigation of cancer therapy side-effects (Zecha et al. 2016a; Zecha et al. 2016b). However in recent years there has been growing interest in the use of PBM in various brain disorders (Hamblin 2016b; Hennessy and Hamblin 2016; Naeser and Hamblin 2011; Naeser and Hamblin 2015). The almost complete lack of any adverse side-effects of PBM, coupled with growing disillusion with pharmaceutical drugs that affect brain function, have combined together to suggest an alternative physical therapy approach to improving brain function.
Traumatic brain injury (TBI) is caused by some type of trauma to the head, often resulting from road traffic accidents, assaults, falls, sports injuries, or blast injuries suffered in military conflict. TBI is classified as mild (loss of consciousness 0-30 minutes; altered mental state <24 hours; post-trauma amnesia <1 day); moderate (loss of consciousness 30 minutes to 24 hours; altered mental state >24 hours; post-trauma amnesia >1-7 days), or severe (loss of consciousness >24 hours; altered mental state >24 hours; post-trauma amnesia >7 days) (Blennow et al. 2016). There are three cases of TBI sustained each minute in the US (Faul et al. 2010). Repeated mild episodes of TBI (also known as concussions) even without loss of consciousness, may have devastating cumulative effects (Kamins and Giza 2016). Chronic traumatic encephalopathy is a recently recognized condition resulting from repeated head trauma, found in boxers, football players, and military personnel (McKee et al. 2016; Safinia et al. 2016). There is presently no accepted treatment for TBI, although some investigational approaches are being tested in both the acute (neuroprotection) and chronic (neurorehabilitation) settings (Loane and Faden 2010). One of these novel approaches is PBM or LLLT (Hamblin 2016a; Hamblin 2016b; Huang et al. 2012; Thunshelle and Hamblin 2016).
Uncertainties about the mechanism of action of PBM at the molecular and cellular levels, have undoubtedly held back its acceptance in the wider biomedical community. However in recent years substantial progress has been made in this regard (de Freitas and Hamblin 2016). In the following section the state-of-the-art knowledge about the mechanisms of PBM is summarized. Figure 1 shows a graphical representation of the cellular and molecular mechanisms of PBM.
Light passes through the scalp and skull, where depending on the wavelength it is absorbed by two different chromophores. Red and NIR (up to 940nm) is primarily absorbed by cytochrome c oxidase in the mitochondrial respiratory chain of the cortical neurons. Longer wavelength NIR light (980nm, 1064nm) is primarily absorbed by heat and light-sensitive transient receptor potential ion channels. In both cases cell signaling and messenger molecules are upregulated as a result of stimulated mitochondrial activity, including reactive oxygen species (ROS), and adenosine triphosphate (ATP). hv is light, TRPV is transient receptor potential vanilloid (ion channels).
2.1 Chromophores
The first law of photobiology states that a photon must be absorbed by some molecule within the tissue to have any biological effect. The identity of these chromophores has been the subject of much scientific investigation and speculation. Largely due to the efforts of Tiina Karu in Russia, the enzyme cytochrome c oxidase (CCO) has been identified as a major chromophore of red/NIR light (Karu 1999; Karu and Kolyakov 2005; Karu et al. 2004a; Karu et al. 2004b). CCO is unit IV in the mitochondrial respiratory chain and has absorption peaks reaching well into the NIR spectral region (up to 900 nm) as well as in the red and blue regions. The most discussed hypothesis to explain exactly how photon absorption can stimulate the activity of CCO involves the photodissociation of inhibitory nitric oxide (NO) that can bind to the copper and heme centers in the enzyme and prevent oxygen from gaining access to the active sites (Lane 2006). In experimental models (such as isolated mitochondria) oxygen consumption and ATP production are increased, and the mitochondrial membrane potential is raised (Passarella et al. 1984).
A less well-appreciated mechanism involves light and heat-gated ion channels. These cation ion channels are thought to be members of the transient receptor potential (TRP) superfamily consisting of over 28 distinct members organized into six subfamilies, based on their primary amino acid structures (Caterina and Pang 2016). TRPV (vanilloid sub-family) members including TRPV1 (capsaicin receptor) have been shown to be activated by various wavelengths of light including green, red and NIR.
2.2 Cellular mechanisms
After the primary photon absorption event occurs, whether that the photons are absorbed by CCO, or by TRP ion channels a series of secondary events occurs. One of these events is the generation of reactive oxygen species (ROS), which are thought to be produced inside the mitochondria due to an increase in electron transport, and a rise in the mitochondrial membrane potential above the baseline levels (Suski et al. 2012). It should be noted that mitochondrial ROS can be produced when MMP is raised above normal, and also when ROS is reduced below normal. It is thought that the ROS produced when MMP is lowered (mitochondrial dysfunction) are more damaging than ROS produced when MMP is raised (mitochondrial stimulation). Nitric oxide is produced after PBM (Hamblin 2008), possibly by photodissociation from CCO where it inhibits oxygen consumption and electron transport (Lane 2006). Cyclic adenosine monophosphate (cAMP) (Gao and Xing 2009) and intracellular calcium are increased (Alexandratou et al. 2002). Many of these secondary mediators in the signaling pathways triggered by PBM, can induce activation of transcription factors, that go on to upregulate or downregulate expression levels of a large number of genes. One of the best-known transcription factors is NF-kB that can regulate expression of over one hundred genes including proteins with antioxidant, anti-apoptotic, pro-proliferation, and pro-migration functions. PBM (810 nm 3J/cm2) was shown to activate NF-kB in mouse embryonic fibroblasts via ROS production (Chen et al. 2011a). Since NF-kB is known to be a pro-inflammatory transcription factor, it might be thought that PBM would be pro-inflammatory. However it was shown that NF-KB was decreased in already activated (treated with Toll-like receptor ligands) inflammatory dendritic cells by PBM (810 nm 3J/cm2) (Chen et al. 2011b).
2.3 Tissue mechanisms
The changes in expression levels of proteins involved in antioxidant and redox-regulation, anti-apoptotic and pro-survival, cellular proliferation, etc mean that distinct changes in tissue homeostasis, healing and regeneration can be expected after PBM. For instance, structural proteins such as collagen are newly synthesized in order to repair tissue damage (Tatmatsu-Rocha et al. 2016). Cells at risk of dying in tissue that has been subjected to ischemic or other insults are protected (Sussai et al. 2010). Stem cells are activated to leave their niche, proliferate and differentiate (Oron and Oron 2016; Zhang et al. 2016). Pain and inflammation are reduced (Chow et al. 2009). Blood flow is increased (Samoilova et al. 2008) (possibly as a result of the release of NO (Mitchell and Mack 2013)), which also stimulates lymphatic drainage thereby reducing edema (Dirican et al. 2011).
2.4 Brain specific mechanisms
In addition to the foregoing, there are some PBM tissue mechanisms that are specific to the brain. One of the most important is an increase in cerebral blood flow often reported after transcranial photobiomodualtion (tPBM) (Salgado et al. 2015), leading to increased tissue oxygenation, and more oxidized CCO as measured by NIR spectroscopy (Rojas and Gonzalez-Lima 2013). tPBM has been shown to reduce activated microglia in the brains of TBI mice as measured by IBA1 (ionized calcium-binding adapter molecule-1) expression thus demonstrating reduced neuroinflammation (Khuman et al. 2012). tPBM has been shown to increase neurogenesis (formation of new brain cells derived from neuroprogenitor cells) (Xuan et al. 2014), and synaptogenesis (formation of new connections between existing brain cells) (Xuan et al. 2015) both in TBI mice. Figure 2 shows a graphical representation of a variety of these brain-specific tissue mechanisms.
The gene transcription process described in Figure 1 can lead to decreases in neuronal apoptosis and excitotoxicity and lessening of inflammation and reduction of edema due to increased lymphatic flow, which together with protective factors such as antioxidants, will all help to reduce progressive brain damage. Increases in angiogenesis, expression of neurotrophins leading to activation of neural progenitor cells and more cell migration, and increased synaptogenesis may all contribute to the brain repairing itself from damage sustained in the trauma. AUC is area under the curve.
Transcranial PBM is a growing approach to many different brain disorders that may be classified as sudden onset (stroke, TBI, global ischemia), neurodegenerative (Alzheimer's, Parkinson's, dementia), or psychiatric (depression, anxiety, posttraumatic stress disorder)(Hamblin 2016b; Hennessy and Hamblin 2016; Thunshelle and Hamblin 2016). In the following section some issues concerning where the light should be delivered, and the effects of PBM on uninjured mice and humans are addressed.
3.1 Light penetration
Several laboratories working in the field of tissue optics, have investigated the penetration of light of different wavelengths though the scalp and the skull, and to what depths into the parenchyma of the brain this light can penetrate. Answering the question “can light shone on the head sufficiently penetrate to reach the brain?” is difficult. The main reason is that at present it is unclear exactly what threshold of power density is necessary (expressed in mW/cm2) at some depth inside the brain to have a biological effect. There clearly must be a minimum value below which, the light can be delivered for an infinite time without having any effect, but whether this threshold is in the region of μW/cm2 or mW/cm2 is unknown at present.
Haeussinger et al. estimated that the mean penetration depth (5% remaining intensity) of NIR light through the scalp and skull was 23.6 + 0:7 mm (Haeussinger et al. 2011). Other studies have found comparable results with some variations depending on the precise location on the head and the precise wavelength studied (Okada and Delpy 2003; Strangman et al. 2014).
Jagdeo et al. (Jagdeo et al. 2012) used human cadaver heads (skull with intact soft tissue) to measure penetration of 830 nm light, and found that penetration depended on the anatomical region of the skull (0.9% at the temporal region, 2.1% at the frontal region, and 11.7% at the occipital region). Tedord et al. (Tedford et al. 2015) also used human cadaver heads to compare penetration of 660 nm, 808 nm, and 940 nm light. They found that 808 nm light penetrated best, and could reach a depth in the brain of 40–50 mm. Lapchak et al. compared the transmission of 810 nm light through the skulls (no soft tissue) of four different species, and found the mouse skull transmitted 40%, while for rat it was 21%, for rabbit it was 11.3 and for the human skull it was only 4.2% (Lapchak et al. 2015). Pitzschke and colleagues compared penetration of 670 nm and 810 nm light into the brain when delivered by a transcranial or a transphenoidal approach, and found that the best combination was 810 nm delivered transphenoidally (Pitzschke et al. 2015). Yaroslavsky et al. examined light penetration of different wavelengths through different parts of the brain tissue (white brain matter, gray brain matter, cerebellum, and brainstem tissues, pons, thalamus). Best penetration was found with wavelengths between 1000 and 1100 nm (Yaroslavsky et al. 2002). Henderson and Morries found that between 0.45% and 2.90% of 810 nm or 980 nm light penetrated through 3 cm of scalp, skull and brain tissue in ex vivo lamb heads (Henderson and Morries 2015a).
3.2 Local vs systemic effects of light
It is possible that the beneficial effects of PBM on the brain cannot be entirely explained by penetration of light through the scalp and skull into the brain itself, at a sufficient intensity to have an effect on the brain cells. The surface power density that can be safely applied to the head, is limited by heating of the skin. Perceptible heating of the skin starts to be felt when the power density is over about 500 mW/cm2, and can become severe at 1 W/cm2.
There has been one study that explicitly addressed whether direct transcranial PBM or indirect PBM is best for the brain. In a study of PBM for Parkinson's disease in a mouse model, Mitrofanis and colleagues compared the direct delivery of light to the mouse head, and they also covered up the head with aluminum foil so that the light was delivered to the remainder of the mouse body. They found that there was a highly beneficial effect on brain histology with light delivered to the head, but nevertheless there was also a statistically significant although less pronounced benefit (referred to as an “abscopal effect”) when the head was shielded from light. Moreover Oron and co-workers (Farfara et al. 2015) have shown that delivering NIR light to the mouse tibia (using either surface illumination or a fiber optic) resulted in improvements in memory and spatial learning in a transgenic mouse model of Alzheimer's disease. They proposed the mechanism involved PBM stimulating c-kit-positive mesenchymal stem cells (MSCs) that were normally resident in autologous bone marrow. These MSCs were proposed to be able to infiltrate the brain, and clear β-amyloid plaques (Oron and Oron 2016). It should be noted in general that the calvarial bone marrow of the skull contains substantial numbers of stem cells (Iwashita et al. 2003).
3.3 PBM for brain in uninjured animals
Several laboratories have reported that shining light onto the head of uninjured healthy mice or rats can improve various cognitive and emotional parameters. The first study reported that exposure of the middle aged (12 months) CD1 female mice to 1072 nm LED arrays (Michalikova et al. 2008) produced improved performance in a 3D maze compared to sham treated age-matched controls. Gonzalez-Lima and coworkers (Gonzalez-Lima and Barrett 2014) showed that transcranial PBM (9 mW/cm2 with a 660 nm LED array) delivered to rats induced dose-dependent increases in oxygen consumption (5% after 1 J/cm2 and 16% after 5 J/cm2) [113]. They also found that tPBM reduced fear renewal and prevented the reemergence of the extinguished conditioned fear-responses (Rojas et al. 2012).
3.4 PBM for enhancement of brain function in uninjured human volunteers
Gonzalez-Lima et al delivered transcranial PBM (1064 nm laser, 60 J/cm2 at 250 mW/cm2) to the forehead in uninjured human volunteers in a placebo-controlled, randomized study. The goal was to improve performance of cognitive tasks related to the prefrontal cortex, including a psychomotor vigilance task (PVT), a delayed match-to-sample (DMS) memory task, and improved mood as measured by the positive and negative affect schedule (PANAS-X) (Barrett and Gonzalez-Lima 2013). Subsequent studies in uninjured humans showed that tPBM with 1064 nm laser could improve performance in the Wisconsin Card Sorting Task (considered the gold standard test for executive function) (Blanco et al. 2015). They also showed that tPBM to the right forehead (but not the left forehead) could improve attention bias modification (ABM) in humans with depression (Disner et al. 2016).
Salgado et al. applied transcranial LED to enhance cerebral blood flow in healthy elderly women, as measured by transcranial Doppler ultrasound (TCD) of the right and left middle cerebral artery and basilar artery. Twenty-five non-institutionalized elderly women (mean age 72 years), with cognitive status > 24, were assessed using TCD before and after transcranial LED therapy. tPBM (627 nm, 70 mW/cm2, 10 J/cm2) was performed at four points of the frontal and parietal region for 30 s each twice a week for 4 weeks. There was a significant increase in the systolic and diastolic velocity of the left middle cerebral artery (25 and 30%, respectively) and the basilar artery (up to 17 and 25%), as well as a decrease in the pulsatility index and resistance index values of the three cerebral arteries analyzed (Salgado et al. 2015).
3.5 PBM for acute stroke
Transcranial PBM delivered to the head, has been investigated as a possible treatment for acute stroke (Lapchak 2010). Animal models such as rats and rabbits, were first used as laboratory models, and these animals had experimental strokes induced by a variety of methods and were then treated with light (usually 810 nm laser) within 24 h of stroke onset (Lampl 2007). In these studies intervention by tLLLT within 24 h had meaningful beneficial effects.
Treatment of acute stroke in human patients was then addressed in a series of three clinical trials called “Neurothera Effectiveness and Safety Trials” (NEST-1 (Lampl et al. 2007), NEST-2 (Huisa et al. 2013), and NEST-3 (Zivin et al. 2014)). The protocol used an 810 nm laser applied to the shaved head (20 separate points in the 10/20 EEG system) within 24 h of patients suffering an ischemic stroke. The first study, NEST-1, enrolled 120 patients between the ages of 40 to 85 years of age and found a significantly improved outcome (p < 0.05 real vs sham, NIH Stroke Severity Scale) 5 days after a single laser treatment had been administered (Lampl et al. 2007). This significantly improved status was still present 90 days post-stroke in 70% of the PBM patients (but only 51% of the sham patients). The second clinical trial, NEST-2, enrolled 660 patients, aged 40 to 90, who were randomly assigned to one of two groups (331 to PBM, 327 to sham) (Zivin et al. 2009). Significant improvements (p < 0.04) were found in the moderate and moderate-severe (but not for the severe) stroke patients. The last clinical trial, NEST-3, was planned for 1000 patients enrolled, but the study was prematurely terminated by the DSMB for futility (an expected lack of statistical significance) (Lapchak and Boitano 2016). Many commentators have asked how tPBM could work so well in the first trial, yet fail in the third trial. Insufficient light penetration, too long an interval between stroke onset and PBM, inappropriate stroke severity measurement scale, use of only one single tPBM treatment, and failure to illuminate different specific areas of the brain for individual patients, have all been suggested as contributory reasons (Hamblin 2016b). It is undoubtedly the case that the failure of NEST-3 has cast a cloud over the whole application of PBMT for TBI as well as for stroke. Many commentators have asked “Why are you testing PBMT for TBI, if it has been shown not to work for stroke?” The failure of the investigators not to take into account the anatomical location of the stroke (and also whether it was deep or superficial) was also likely to have played a role in the failure of NEST-3. It is logical that light should be applied to the same side of the head where the lesion was located, not both sides of the head (Naeser et al. 2012). In my opinion the use of a single application of PBMT also bore some of the responsibility. Although a single application of PBM to the head works very well for experimental animals (mice, rats, rabbits) who have suffered a stroke or a TBI, the same may not apply to humans.
Oron's group was the first (Oron et al. 2007) to demonstrate that a single exposure of the head of a mouse a few hours after creation of a TBI lesion using a NIR laser (808 nm) could improve neurological performance and reduce the size of the brain lesion. A weight-drop device was used to induce a closed-head TBI in the mice. An 808 nm diode laser with two energy densities calculated at the surface of the brain (1.2-2.4 J/cm2 delivered by 2 minutes of irradiation with 200mW laser power to the scalp) was delivered to the head 4 hours after TBI was induced. Neurobehavioral function was assessed by the neurological severity score (NSS). There was no significant difference between the control and laser-treated group in NSS between the power densities (10 vs 20 mW/cm2), and no significant difference at early time points (24 and 48 hours) post TBI. However, there was a significant improvement (27% lower NSS score) in the PBM group at times between 5 days and 4 weeks. The laser treated group also showed a smaller loss of cortical tissue than the sham group (Oron et al.). In another study (Oron et al. 2012) they varied the pulse parameters (CW, 100Hz, or 600Hz) and tested whether the tPBM was equally effective when delivered at 4, 6, or 8 hours post-TBI. They first established that a calculated dose to the cortical surface of 1.2 J/cm2 of 808nm laser at 200mW applied to the head, was more effective when delivered at 6 hours post TBI than at 8 hours. They then selected an even shorter time post-TBI (4 hours) and compared CW with 100Hz and 600Hz. At 56 days, more mice in the 100Hz group (compared to the CW and 600 Hz groups) had fully recovered. The 600Hz group had lower NSS scores than the CW and 100Hz groups up to 20 days. Magnetic resonance imaging (MRI) analysis demonstrated significantly smaller lesion volumes in PBM-treated mice compared to controls.
4.2 Studies from the Hamblin laboratory
Wu et al. (Wu et al. 2012) first explored the effect of varying the laser wavelengths of PBM had on closed-head TBI in mice. Mice were randomly assigned to a PBM treatment group with a particular wavelength, or to a sham treatment group as a control. Closed-head injury (CHI) was induced via a weight- drop apparatus. To analyze the severity of the TBI, the neurological severity score (NSS) was measured and recorded. The injured mice were then treated with varying wavelengths of laser light (665, 730, 810 or 980 nm) at an energy density of 36 J/cm2 directed onto the scalp at 4 hours post-TBI. The 665 nm and 810 nm laser groups showed significant improvement in NSS when compared to the control group between days 5 to 28. By contrast, the 730 nm and 980 nm laser groups did not show any significant improvement in NSS (Wu et al. 2012) (Figure 3). The tissue chromophore cytochrome c oxidase (CCO) is proposed to be responsible for the underlying photon absorption process that underlies many PBM effects. CCO has absorption bands around 665 nm and 810 nm while it has a low absorption region at the wavelength of 730 nm (Karu et al.). It should be noted that this particular study (Wu et al. 2012) found that the 980 nm did not produce the same positive effects as the 665 nm and 810 nm wavelengths did; nevertheless previous studies did find that the 980 nm wavelength was an active one for PBM (Anders et al. 2014). Wu et al. suggested that these dissimilar results may be due to differences in the energy density, irradiance etc. between the other studies and the Wu study (Wu et al. 2012). In particular a much lower dose of 980 nm might have been effective had it been tested (Wang et al. 2016). Ando et al. (Ando et al. 2011) next used the 810 nm wavelength produced by a Ga-Al-As diode laser delivered at parameters used in the Wu study, and varied the pulse modes of the laser. These modes consisted of either pulsed wave at 10 Hz or at 100 Hz (50% duty cycle) or continuous wave laser. They used a different mouse model of TBI induced with a controlled cortical impact device directly inflicting a lesion on the cortex via an open craniotomy. A single treatment with a power density of 50 mW/m2 and an energy density of 36 J/cm2 (duration of 12 minutes) was given via tLLLT to the closed head in mice at 4 hours post CCI. At 48 hours to 28 days post TBI, all laser treated groups had significant decreases in the measured neurological severity score (NSS) when compared to the controls. Although all laser treated groups had similar NSS improvement rates up to day 7, the PW 10 Hz group began to show even greater improvement beyond this point as seen in Figure 4. At day 28, the forced swim test for depression and anxiety was used and showed a significant decrease in the immobility time for the PW 10 Hz group. In the tail suspension test, which measures depression and anxiety, there was also a significant decrease in the immobility time at day 28, and also at day 1, in the PW 10 Hz group.
Effect of different laser wavelengths of tPBM in closed-head TBI in mice
(A) Sham-treated control versus 665 nm laser. (B) Sham-treated control versus 730 nm laser. (C) Sham-treated control versus 810 nm laser. (D) Sham-treated control versus 980 nm laser. Points are means of 8–12 mice and bars are SD. *P < 0.05; **P < 0.01; ***P < 0.001 (one-way ANOVA). Reprinted with permission from (Wu et al. 2012)
(A) Time course of neurological severity score (NSS) of mice with TBI receiving either control (no laser-treatment), or 810 nm laser (36 J/cm2 delivered at 50 mW/cm2 with a spot size of 0.78 cm2 in either CW, PW 10 Hz or PW 100 Hz modes. Results are expressed as mean +/- S.E.M ***P < 0.001 vs. the other conditions. (B) Mean areas under the NSS-time curves in the two-dimensional coordinate system over the 28-day study for the 4 groups of mice. Results are means +/- SD (n = 10). Reprinted from (Ando et al. 2011) (open access).
Studies using immunofluorescence staining of sections cut from mouse brains showed that tPBM increased neuroprogenitor cells (incorporating BrdU) in the dentate gyrus (DG) of the hippocampus and the subventricular zone (SVZ) at 7 days after the treatment (Xuan et al. 2014). The neurotrophin known as brain derived neurotrophic factor (BDNF) was also increased in the DG and SVZ at 7 days, while the protein marker (synapsin-1) for synaptogenesis and neuroplasticity was increased in the cortex at 28 days but not in the DG, SVZ or in any location at 7 days (Xuan et al. 2015). Learning and memory as measured by the Morris water maze was also improved by tPBM (Xuan et al. 2014).
4.3 Studies from the Wu laboratory
Zhang et al. (Zhang et al. 2014) first showed that secondary brain injury occurred to a worse degree in mice that had been genetically engineered to lack “Immediate Early Response” gene X-1 (IEX-1). When these mice were exposed to a gentle head impact (thought to closely resemble mild TBI in humans) they had a worse NSS than uninjured mice with the same TBI. Exposure of IEX-1 knockout mice to PBM (150 mW/cm2, 4 min, and 36 J/cm2) delivered at 4 hours post injury, restored the NSS to almost baseline levels, suppressed proinflammatory cytokine expression of interleukin (IL)-Iβ and IL-6, but upregulated TNF-α. The original lack of IEX-1 decreased ATP production, but exposing the injured brain to LLLT elevated ATP production back to near normal levels.
Dong et al. (Dong et al. 2015) asked whether the beneficial effects of PBM on TBI in mice could be enhanced by combining PBM with administration of metabolic substrates such as pyruvate and/or lactate. The goal was to even further improve mitochondrial function in the brain. This combinatorial treatment was able to reverse memory and learning deficits in TBI injured mice back to normal levels as well as leaving the hippocampal region completely protected from tissue loss; a stark contrast to control TBI mice that exhibited severe tissue loss from secondary brain injury.
4.4 Studies from the Whalen laboratory
Khuman et al (Khuman et al. 2012) delivered PBM (800nm) either directly to the injured brain tissue (through the craniotomy) or transcranially in mice beginning 60-80 min after CCI TBI. At a dose of 60J/cm2 (500mW/cm2) the mice showed increased performance in the Morris water maze (latency to the hidden platform, p<0.05, and probe trial, p<0.01) compared to non-treated controls. When PBM was delivered via open craniotomy there was reduced microgliosis at 48h (IbA-1+ cells, p<0.05). Little or no effect of tPBM on post-injury cognitive function was observed using lower or higher doses, a 4-h administration time point or 60J/cm2 at 7-days post-TBI.
4.5 Studies from the Whelan laboratory
Quirk et al (Quirk et al. 2012) studied Sprague-Dawley rats who had received a severe CCI TBI and were divided into three groups: real TBI, sham surgery, and anesthetization only. Each group received either real or sham PBM consisting of 670nm LED treatments of 15J/cm2, 50mW/cm2, 5min, given two times per day for 3 days (chemical analysis) or 10 days (behavioral analysis using a TruScan nose-poke device). Significant differences in task entries, repeat entries, and task errors were seen in the TBI rats treated with PBM vs untreated TBI mice, and in sham surgery mice treated with PBM vs untreated sham surgery mice. A statistically significant decrease was found in the pro-apoptotic marker Bax, and increases in the anti-apoptotic marker Bcl-2 and reduced glutathione (GSH) levels in tPBM TBI mice.
4.6 Studies from the Marques laboratory
Moreira et al used a different model of TBI (Moreira et al. 2009). Wistar rats received a craniotomy and a copper probe cooled in liquid nitrogen was applied to the surface of the brain to create a standardized cryogenic injury. They treated the rats with either a 780nm or 660nm laser at one of two different doses (3J/cm2 or 5J/cm2) twice (once immediately after the injury and again 3 hours later). Rats were sacrificed 6h and 24h after the injury. The 780nm laser was better at reducing levels of pro-inflammatory cytokines (TNFα, IL1β, IL6) particularly at early timepoints (Moreira et al. 2009). In a follow-up study using 3 J/cm2 (Moreira et al. 2011) these workers reported on the healing of the injuries in these rats at timepoints 6h, 1, 7 and 14 days after the last irradiation. Cryogenic injury created focal lesions in the cortex characterized by necrosis, edema, hemorrhage and inflammatory infiltrate. The most striking findings were: PBM-treated lesions showed less tissue loss than control lesions at 6h. During the first 24h the amount of viable neurons was significantly higher in the PBM groups. PBM reduced the amount of GFAP (glial fibrillary acidic protein, a marker of astrogliosis) and the numbers of leukocytes and lymphocytes, thus demonstrating its anti-inflammatory effect.
The majority of studies of PBM for TBI in laboratory animals have been conducted in the acute setting, while the majority of human studies of PBM for TBI have been conducted in patients who have suffered head injuries at various times in the past (sometimes quite a long time ago).
5.1 Naeser case reports
In 2011 Naeser, Saltmarche et al., published the first report describing two chronic, TBI cases treated with tPBM (Naeser et al. 2011). A 500 mW CW LED source (mixture of 660 nm red and 870 nm NIR LEDs) with a power density of 22.2 mW/cm2 (area of 22.48 cm2), was applied all over the head, for 10 minutes at each placement location (13.3 J/cm2). In the first case study the patient reported that she could concentrate on tasks for a longer period of time (the time able to work at a computer increased from 20 minutes to 3 hours). She had a better ability to remember what she read, decreased sensitivity when receiving haircuts in the spots where PBM was applied, and improved mathematical skills after undergoing PBM. The second patient had statistically significant improvements compared to prior neuropsychological tests after 9 months of treatment. The patient had a 2 standard deviation (SD) increase on tests of inhibition and inhibition accuracy (9th percentile to 63rd percentile on the Stroop test for executive function and a 1 SD increase on the Wechsler Memory scale test for the logical memory test (83rd percentile to 99th percentile) (Naeser et al. 2011).
5.2 Naeser case series
Naeser et al then went on to report a case series containing a further eleven patients (Naeser et al. 2014). This was an open protocol study that examined whether scalp application of red and NIR LED could improve cognition in patients with chronic, mild TBI (mTBI). This study enrolled 11 participants ranging in age from 26 to 62 years (6 males, 5 females) who suffered from persistent cognitive dysfunction after mTBI. The injuries in the participants had been caused by motor vehicle accidents, sports related events and for one participant, an improvised explosive device (IED) blast. tPBM consisted of 18 sessions (Monday, Wednesday, and Friday for 6 weeks) and was started anywhere from 10 months to 8 years post-TBI. A total of 11 LED cluster heads (5.25 cm in diameter, 500 mW, 22.2 mW/cm2, 13 J/cm2) were applied for 10 minutes per set (5 or 6 LED placements per set, Set A and then Set B, in each session). Neuropsychological testing was performed pre-LED application and 1 week, 1 month and 2 months after the final treatment. They found that there was a significant positive linear trend for the Stroop Test for executive function, in trial 3 inhibition (p = 0.004); Stroop, trial 4 inhibition switching (p = 0.003); California Verbal Learning Test (CVLT)-II, total trials 1-5 (p = 0.003); CVLT-II, long delay free recall (p = 0.006). Improved sleep and fewer post-traumatic stress disorder (PTSD) symptoms, if present beforehand, were observed after treatment. Participants and family members also reported better social function and a better ability to perform interpersonal and occupational activities. Although these results were significant, the authors suggested that further placebo-controlled studies would be needed to ensure the reliability of this approach (Naeser et al. 2014).
Naeser has proposed (Naeser et al. 2016; Naeser et al. 2014) that specific scalp placements of the LED cluster heads may affect specific cortical nodes in the intrinsic networks of the brain, such as the default mode network (DMN), the salience network (SN), and the central executive network (CEN). These intrinsic networks are often dysregulated after TBI (Sharp et al. 2014). Naeser proposed that the specific areas of the head to receive light, to target cortical nodes in these networks were as follows:
For the DMN, placement of the LED cluster head on the midline of face, centered on the upper forehead and the front hairline, targeted the left and right mesial prefrontal cortex; and on a midline, scalp location half-way between the occipital protuberance and the vertex of the head, targeted the precuneus; and on left and right LED placements superior to the tip of each ear and posterior to each ear, targeted the inferior parietal cortex/angular gyrus areas.
For the SN, placement of LED cluster heads on the left and right temple areas, to target the anterior insula (but due to depth of insula, unknown if the photons reached the target); midline of the vertex of the head, to target the left and right presupplementary motor areas; and the LED cluster head placed on the midline of face, centered on the upper forehead and the front hairline, also targeted the left and right dorsal anterior cingulate cortex.
For the CEN, left and right scalp LED placements immediately posterior to the front hairline (on a line directly superior from the pupils of the eyes), targeted the dorso-lateral prefrontal cortex areas; and the left and right LED placements superior to the tip of each ear and posterior to each ear, also targeted the posterolateral inferior parietal cortex/angular gyrus areas (also treated as part of the DMN).
Further studies from Naeser and colleagues (Naeser et al. 2016) tested an intranasal LED (iLED) device. Two small iLEDs (one red and the other NIR) were clipped into each nostril and used at the same time for 25 min. The parameters were as follows: red, 633nm, 8mW CW, 1 cm2, energy density 12 J/cm2 (25 min); NIR 810nm, 14.2mW, pulsed 10Hz, 1cm2, 21.3J/cm2. The first mTBI participant (24-year old female) who had sustained four sports-related concussions (two during snowboarding and two during field hockey), received iLED PBM three times per week for 6 weeks. Significant improvements were observed in tasks measuring executive function and verbal memory as well as attention and verbal fluency. At 1 week after the 18th iLED treatment, the average total time asleep had increased by 61 min per night and her sleep efficiency (total sleep time divided by total time in bed) had increased by 11%. At 12 weeks after the last iLED treatment, she was able to discontinue all sleep medications that she had previously been using. The second, mTBI participant who received the intranasal only, LED treatment series is a 49 Yr. M (non-Veteran) who sustained mTBI in a MVA, 30 years prior to receiving the intranasal LED treatment series. He showed significant improvement on the Controlled Oral Word Association-FAS Test post- the iLED treatment series, improving by +1.3 SD and +1.5 SD at 1 and 2 months post- the 18th iLED treatment. His sleep data indicated he was already a good sleeper, at entry.
5.3 Bogdanova and Naeser studies
Bogdanova reported (Bogdanova et al. 2014) a case report of two patients (1 female) with moderate TBI (medical records and clinical evaluation) and persistent cognitive dysfunction (as measured by neuropsychological tests of executive function and memory). Patients received 18 sessions of transcranial LED therapy (3×/week for 6 weeks) using the mixed red/NIR cluster described above (Naeser et al. 2011).
Standardized neuropsychological tests for executive function, memory, depression, PTSD and sleep measures (PSQI, actigraphy) were administered to participants pre-(T1), mid-(T2), and one week (T3) post-PBM treatment. Both PBM treated cases (P1 and P2) showed marked improvement in sleep (actigraphy total sleep) 1 week post-LED treatment (T3), as compared to pre-treatment (T1). P1 also improved in executive function, verbal memory, and sleep efficiency; while P2 significantly improved on measures of PTSD (PCL-M) and depression. No adverse events were reported.
5.4 Studies from Henderson and Morries
Henderson and Morries (Henderson and Morries 2015b) used a high-power NIR laser (10-15 W at 810 and 980 nm) and applied it to the head to treat a patient with moderate TBI. The patient received 20 NIR applications over a 2-month period. They carried out anatomical magnetic resonance imaging (MRI) and perfusion single-photon emission computed tomography (SPECT). The patient showed decreased depression, anxiety, headache, and insomnia, whereas cognition and quality of life improved, accompanied by changes in the SPECT imaging.
They next reported (Morries et al. 2015) a series of ten patients with chronic TBI (average time since injury 9.3 years) where each patient received ten treatments over the course of 2 months using a high-power NIR laser (13.2 W/0.89 cm2 equivalent to 14.6 W/cm2 at 810nm; or 9 W/0.89 cm2 equivalent to 10.11 W/cm2 at 980nm). A continuous sweeping motion over the forehead was utilized to minimize skin heating and cover a larger area. Skin temperature increased no more than 3°C. Overall symptoms of headache, sleep disturbance, cognition, mood dysregulation, anxiety, and irritability improved. Symptoms were monitored by depression scales and a novel patient diary system specifically designed for this study. These authors have proposed that high power lasers are preferable for tPBM treatments because the photons can better reach the brain (Henderson and Morries 2015a).
5.5 Case study from Nawashiro
Nawashiro et al (Nawashiro et al. 2012) treated a single patient who had suffered a severe TBI. The patient survived but was left in a persistent vegetative state for 8 months after the accident. He showed no spontaneous movement of limbs and a CT scan of the head 8 months after the accident showed a focal low-density area in the right frontal lobe. The device had 23 individual 850nm LEDs (13mW each; total power 299mW, total area 57cm2). A treatment time of 30 min per session delivered 20.5 J/cm2 over the left and right forehead areas repeated twice daily (6h apart), for 73 days. Five days after beginning the PBM (after 10 treatments), the patient began to spontaneously move his left arm and hand, which had not occurred during the previous 8 months. Single-photon emission computed tomography with N-isopropyl-[123I]p-iodoamphetamine (IMP-SPECT) was performed twice. The IMP-SPECT scans showed a focal increase (20% higher) in cerebral blood flow in the uninjured left anterior frontal lobe 30 min after the last (146th) PBM treatment, compared to before PBM began.
As was mentioned above, one of the most important questions to be answered when contemplating clinical treatment of TBI patients with tPBM, is what is the best time to administer the treatment? All the available reports of studies using PBM in laboratory animal models of TBI and stroke, and also in patients treated for stroke, have been in the acute phase where the overall goal of the intervention can be best described as neuroprotection. Not only that but there are several reports (Lapchak et al. 2007; Oron et al. 2012) that PBM for both TBI and stroke is most effective when it is delivered as soon as possible after the actual event (head impact or ischemic stroke). The protocols for the series of NEST clinical trials specified that patients should be treated with PBM within 24 hours of the stroke occurring. By contrast, all the clinical trials of PBM for patients with TBI, that have so far been carried out, have been with chronic TBI, after varying periods of time having elapsed after the original head injury, sometimes as long as 8 years. Although it would be generally supposed that tPBM would be effective when delivered to acute TBI patients, this has not yet been actually tested. If tPBM were to be used for acute TBI patients, then presumably the PBM should be delivered perhaps beginning at 4 to 6 hours post-TBI, for a limited number of times after the injury; perhaps once a day for 7 days?
The dosimetry and optimum delivery apparatus of tPBM is still uncertain. Although there is some consensus that wavelengths in the region of 800-900nm will penetrate the scalp and skull, other workers have used longer NIR wavelengths, 980nm, 1064nm, or 1072nm. Pulsing or CW is another unresolved question. The exact locations on the head that should receive the light are still unknown. Naeser has proposed (Naeser et al. 2016) some interesting considerations regarding the scalp placements of the tLEDS, and their effect on various intrinsic cortical networks of the brain. Targeted LED placements could promote better neuromodulation (activation/deactivation) in specific cortical nodes. It is possible that communication between nodes within one single network, and/or across networks could be improved. Moreover preliminary data indicate that intranasal, red plus near-infrared LEDs can also benefit TBI patients, although the degree to which light incident on the nasal mucosa, and possibly delivered transsphenoidally (Pitzschke et al. 2015) can penetrate directly into the brain, remains to be determined.
An advantage of intranasal and/or transcranial LED PBM therapy is that it can be performed in the home, for long-term use (Naeser et al. 2011). Also, 5 chronic, mild to moderately-severe dementia cases recently showed significant improvement on the Mini-Mental State Examination (p<0.003), and on the Alzheimer's Disease Assessment Scale-Cognitive subscale (p<0.023) after 12 weeks of daily, at-home, intranasal, near-infrared LED PBM treatments (810nm, pulsed at 10 Hz), and once-a-week in-office, tLED treatments applied to the cortical nodes of the Default Mode Network (Saltmarche et al. 2017). Anecdotally, there was also improved sleep, fewer angry outbursts, and less wandering. When all LED treatments were withdrawn after 12 weeks of active LED PBM treatment, there was precipitous decline in cognition and behavior. Thus, at-home, long-term use of iLED plus tLED PBM offers a potential therapy to mitigate the sequelae of Alzheimer's disease and possibly other neurodegenerative disorders, as well as TBI and stroke.
One highly distressing aspect of TBI symptomatology that has not so far been addressed by PBM, is that of post-traumatic epilepsy (PTE). TBI is the most significant cause of symptomatic epilepsy in people from 15 to 24 years of age. The frontal and temporal lobes are the most frequently affected regions, but imaging (MRI) often fails to show the precise cause. During PTE seizures there is an abnormal electrical discharge in the brain, with staring and unresponsiveness, stiffening or shaking of the body, legs, arms or head; strange sounds, tastes, visual images, feelings or smells; inability to speak or understand, etc (Cotter et al. 2017). Epilepsy has traditionally been considered to be a contra-indication for PBMT (Navratil and Kymplova 2002). However the knowledge that has recently been gained concerning the beneficial effects of PBMT on the damaged brain, suggests that this view may need to be critically revisited.
Moreover there is also potential of tPBM to treat a wide range of brain disorders only loosely associated with TBI, including Parkinson's disease (Purushothuman et al. 2013), depression, anxiety, post-traumatic stress disorder, autism spectrum disorder and so on (Hamblin 2016b).
The ongoing and accelerating clinical research efforts in testing PBM for TBI, are expected to lead to the answering of many of these questions in the coming years.
Hashmi JT1, Huang YY, Sharma SK, Kurup DB, De Taboada L, Carroll JD, Hamblin MR. - Lasers Surg Med. 2010 Aug;42(6):450-66. doi: 10.1002/lsm.20950. (Publication) 2004 This is one of the most complete review of pulsed lasers versus continuous wave lasers. They also try to determine if there is a best pulsing frequency.
Since the introduction of low-level laser (light) therapy in 1967, over two hundred randomized, double-blinded, and placebo-controlled phase III clinical trials have been published from over a dozen countries. Whereas there is some degree of consensus as to the best wavelengths of light and acceptable dosages to be used, there is no agreement on whether continuous wave (CW) or pulsed wave (PW) light is more suitable for the various applications of LLLT. This review will raise (but not necessarily answer) several questions. How does pulsed light differ from CW on the cellular and molecular level, and how is the outcome of LLLT affected? If pulsing is more efficacious, then at what pulse parameters is the optimal outcome achieved? In particular, what is the ideal pulse repetition rate or frequency to use?
PULSE PARAMETERS AND LIGHT SOURCES
There are five parameters that could be specified for pulsed light sources. The pulse width or duration or ON time (PD) and the pulse Interval or OFF time (PI) are measured in seconds. Pulse repetition rate or frequency (F) is measured in Hz. The duty cycle (DC) is a unitless fractional number or %. The peak power and average power are measured in Watts.
Pulse duration, pulse repetition rate, and duty cycle are related by the simple equation:
DC=F×PD
Peak power is a measure of light intensity during the pulse duration, and related to the average power (measured in Watts) by:
Average power=Peak power×F×PD
Alternatively,
Peak power=Average powerDC
In all cases, it is necessary to specify any two out of three of: PD, F, and DC, and either the peak or average power for the pulse parameters to be fully defined.
Figure 1 graphically shows the relationship between peak power and pulse duration.
Five major types of pulsed lasers (or other light sources) are commonly utilized: (1) Q-switched, (2) Gain-switched, (3) Mode-locked, (4) Superpulsed, and (5) Chopped or gated. Each utilizes a different mechanism to generate light in a pulsed as opposed to continuous manner, and vary in terms of pulse repetition rates, energies, and durations. However the first three classes of “truly” pulsed lasers mentioned above are in general not used for LLLT; instead superpulsed or gated lasers are mainly used. The concept of super-pulsing was originally developed for the carbon dioxide laser used in high power tissue ablative procedures. The idea was that by generating relatively short pulses (µsecond) the laser media could be excited to higher levels than those normally allowed in CW mode where heat dissipation constraints limit the maximum amounts of energy that can be used to excite the lasing media. With the original carbon dioxide superpulsed lasers, the short pulses would confine the thermal energy in the tissue (by making the pulse duration less than the thermal diffusion time) reducing collateral thermal damage to normal tissue.
Another type of laser that particularly benefited from super-pulsing is the gallium-arsenide (GaAs) diode laser. This laser has a wavelength in the region of 904-nm and pulse duration usually in the range of 100–200 nanoseconds. Another semiconductor laser amenable to superpulsing is the indium-gallium-arsenide (In-Ga-As) diode laser. It emits light at a similar wavelength (904–905-nm) as the GaAs diode laser, producing very brief pulses (200 nanoseconds) of high frequencies (in the range of kilohertz). These pulses are of very high peak powers (1–50 W) and an average power of 60 mW. Theoretically, the super-pulsed GaAs and In-Ga-As lasers allow for deep penetration without the unwelcome effects of CW (such as thermal damage), as well as allowing for shorter treatment times.
The other major class of pulsed light sources used in LLLT are simply CW lasers (usually diode lasers) that have a pulsed power supply generated by a laser driver containing a pulse generator. This technology is described as “chopped” or “gated.” It is also equally feasible to use pulse generator technology to pulse LEDs or LED arrays [1].
WHY COULD PULSING BE IMPORTANT IN LLLT?
Pulsed light offers numerous potential benefits. Because there are “quench periods” (pulse OFF times) following the pulse ON times, pulsed lasers can generate less tissue heating. In instances where it is desirable to deliver light to deeper tissues increased powers are needed to provide adequate energy at the target tissue. This increased power can cause tissue heating at the surface layers and in this instance pulsed light could be very useful. Whereas CW causes an increase in temperature of the intervening and target tissues or organ, pulsed light has been shown to cause no measurable change in the temperature of the irradiated area for the same delivered energy density. Anders et al. administered pulsed light to pig craniums, and found no significant change in temperature of the scalp or skull tissue (J.J. Anders, personal communication). Ilic et al. [2] found that pulsed light (peak power densities of 750 mW/cm2) administered for 120 seconds produced no neurological or tissue damage, whereas an equal power density delivered by CW (for the same number of seconds) caused marked neurological deficits.
Aside from safety advantages, pulsed light might simply be more effective than CW. The “quench period” (pulse OFF times) reduces tissue heating, thereby allowing the use of potentially much higher peak power densities than those that could be safely used in CW. For example, when CW power densities at the skin of ≥2 W/cm2 are used, doubling the CW power density would only marginally increase the treatment depth while potentially significantly increasing the risk of thermal damage; in contrast, peak powers of ≥5 W/cm2 pulsed using appropriate ON and OFF times might produce little, or no tissue heating. The higher peak powers that can be safely used by pulsing light can overcome tissue heating problems and improve the ability of the laser to penetrate deep tissues achieving greater treatment depths.
There may be other biological reasons for the improved efficacy of pulsed light (PW) over CW. The majority of the pulsed light sources used for LLLT have frequencies in the 2.5–10,000 Hz range and pulse durations are commonly in the range of a few millisecond. This observation suggests that if there is a biological explanation of the improved effects of pulsed light it is either due to some fundamental frequency that exists in biological systems in the range of tens to hundreds of Hz, or alternatively due to some biological process that has a time scale of a few milliseconds. Two possibilities for what these biological processes could actually be occur to us. Firstly, it is known that mammalian brains have waves that have specific frequencies [3]. Electroencephalography studies have identified four distinct classes of brain waves [4,5]. Alpha waves (8–13 Hz) occur in adults who have their eyes closed or who are relaxed [6]. Beta waves (14–40 Hz) mainly occur in adults who are awake, alert or focused [7]. Delta waves (1–3 Hz) occur mainly in infants, adults in deep sleep, or adults with brain tumors [8]. Theta waves (4–7 Hz) occur mainly in children ages 2–5 years old and in adults in the twilight state between sleeping and waking or in meditation [9]. The possibility of resonance occurring between the frequency of the light pulses and the frequency of the brain waves may explain some of the results with transcranial LLLT using pulsed light.
Secondly, there are several lines of evidence that ion channels are involved in the subcellular effects of LLLT. Some channels permit the passage of ions based solely on their charge of positive (cationic) or negative (anionic) while others are selective for specific species of ion, such as sodium or potassium. These ions move through the channel pore single file nearly as quickly as the ions move through free fluid. In some ion channels, passage through the pore is governed by a “gate,” which may be opened or closed by chemical or electrical signals, temperature, or mechanical force, depending on the variety of channel. Ion channels are especially prominent components of the nervous system. Voltage-activated ion channels underlie the nerve impulse and while transmitter-activated or ligand-gated channels mediate conduction across the synapses.
There is a lot of literature on the kinetics of various classes of ion channels but in broad summary it can be claimed that the time scale or kinetics for opening and closing of ion channels is of the order of a few milliseconds. For instance Gilboa et al. [10] used pulses having a width 10 milliseconds and a period of 40 milliseconds (25 Hz). Other reports on diverse types of ion channels have given kinetics with timescales of 160 milliseconds [11], 3 milliseconds [12] and one paper giving three values of 0.1, 4 and 100 milliseconds [13]. Potassium and calcium ion channels in the mitochondria and the sarcolemma may be involved in the cellular response to LLLT [14–16].
Thirdly there is the possibility that one mechanism of action of LLLT on a cellular level is the photodissociation of nitric oxide from a protein binding site (heme or copper center) such as those found in cyctochrome c oxidase [17]. If this process occurs it is likely that the NO would rebind to the same site even in the presence of continuous light. Therefore if the light was pulsed multiple photodissociation events could occur, while in CW mode the number of dissociations may be much smaller.
PENETRATION DEPTH
The most important parameter that governs the depth of penetration of laser light into tissue is wavelength. Both the absorption and scattering coefficients of living tissues are higher at lower wavelength so near-infrared light penetrates more deeply that red and so on. It is often claimed that pulsed lasers penetrate more deeply into tissue than CW lasers with the same average power. Why exactly should this be so? Let us suppose that at a certain wavelength (for instance 810-nm) the depth of tissue at which the intensity of a laser is reduced to 10% of its value at the surface of the skin is 1-cm. Therefore if we are using a laser with a power density (irradiance) of 100 mW/cm2 at the skin, the power density remaining at 1 cm below the skin is 10 mW/cm2 and at 2-cm deep is 1 mW/cm2. Now let us suppose that a certain threshold power density (minimum number of photons per unit area per unit time) at the target tissue is necessary to have a biological effect and that this value is 10 mW/cm2. The effective penetration depth at CW may be said to be 1-cm. Now let us suppose that the laser is instead pulsed with a 10-milliseconds pulse duration at a frequency of 1 Hz (DC = 1 Hz×0.010 seconds = 0.010) and the same average power. The peak power and peak power densities are now 100 times higher (peak power = average power/DC = average power×100). With a peak power density of 10 W/cm2 at the skin, the tissue depth—at which this peak power density is attenuated to the threshold level of 10 mW/cm2—is now 3-cm rather than 1-cm in CW mode. But what we have to consider is that the laser is only on for 1% of the time so the total fluence delivered to the 3-cm depth in pulsed mode is 100 times less than that delivered to 1-cm depth in CW mode. However it would be possible to increase the illumination time by a factor of 100 to reach the supposed threshold of fluence as well as the threshold of power at the 3-cm depth. In reality the increase in effective penetration depth obtained with pulsed lasers is more modest than simple calculations might suggest. Many applications of LLLT do not require deep penetration such as tendinopathies and joint pain.
Similarly, deep penetration is often not required to alleviate joint pain. The target tissue in such cases is the synovia; with the exception of back, neck, and hip, most joints have readily accessible synovia. Bjordal et al. [19] conducted a review of literature and concluded that “superpulsed” lasers (904 nm) were not significantly more effective than CW lasers (810–830 nm); both types of laser achieved similar results, but half the energy was needed to be used for superpulsed lasers. On the other hand, deeper penetrance is needed to reach back, neck, and hip joints. If power densities greater than a few mW/cm2 are to be safely delivered to target tissues >5 cm below the skin, it appears likely that this can only be done by using pulsed lasers. It is postulated that successful LLLT treatments in such joints bring benefit not by reaching the deep target tissue but by inhibiting superficial nociceptors. In other words, they bring relief primarily by attenuating pain perception, as opposed to decreasing inflammation. Does deeper penetration via pulsed lasers offer any significant benefit over CW? It is quite possible that a relatively higher fluence is necessary to attenuate pain, whereas a lower fluence decreases inflammation. If this is indeed the case, for musculo-skeletal applications achieving higher doses at the level of the target tissue may not be ideal. Further studies must be done to confirm this hypothesis, as well as to determine if there is any real benefit to the deeper penetration attained by pulsed lasers. Muscles such as the biceps and rectus femoris are not small organs, and have quite deep target tissue. Yet, various studies have shown significant improvement with CW lasers and CW LED. It remains to be seen whether or not pulsed lasers offer any additional advantage. Similarly, depression [20] and stroke studies [21] using LLLT have demonstrated that CW LED’s and CW lasers (respectively) produce a beneficial therapeutic effect. There are reports from Anders’ laboratory that fluences as low as 0.1–0.2 J/cm2 may be optimal for cells in the brain [22]. However, further studies must be done to determine whether pulsed light, with higher peak power densities deeper into the brain tissues, might increase the effectiveness of these therapies.
STUDIES COMPARING CW AND PW
In this review thirty-three studies involving pulsed LLLT were examined. Of these studies, nine of them directly compared continuous wave (CW) with pulsed wave (PW) light, as recorded in Table 1. Six of these nine studies found PW to be more effective than CW. One study comparing CW and PW found both modes of operation to be equally effective, with no statistically significant difference between the two. Only two of the nine articles reported better results with CW than PW, although in both of these studies PW treated subjects were found to have better outcomes than placebo groups. One of the recurring limitations of the papers in this review was that like for like irradiation parameters were not used. For instance, Gigo-Benato et al. [23] found CW superior to PW in nerve regeneration, but is this because of the mode of operation (CW or PW) or because the CW laser used 808 nm and the pulsed laser used 905 nm?
Of the six studies that found PW to be more effective than CW, four of them involved the use of LLLT to cure the following pathologies in vivo: wound healing, pain, and ischemic stroke. The two remaining studies reported pulsing to be beneficial in vitro; in the first such study, PW promoted bone stimulation more so than CW. The other in vitro study comparing CW and PW found the latter mode of operation better able to penetrate through melanin filters, indicating that pulsing may be beneficial in reaching deep target tissue in dark-skinned patients.
In the wound healing study, Kymplova et al. [24] used a large sample size of women to study the effects of phototherapy on wound repair following surgical episiotomies (one of the most common surgical procedures in women). A pulsed laser emitted light (wavelength of 670 nm) at various frequencies (10, 25, and 50 Hz). The pulsed laser promoted wound repair and healing more so than the CW light source.
In the pain study, Sushko et al. [25] investigated the role of pulsed LLLT to attenuate pain in white male mice. The same wavelength of light was used as in Kymplova et al.’s study (670 nm), with the frequencies of 10, 600, and 8,000 Hz. Both modes of delivery (CW and PW) reduced the behavioral manifestations of somatic pain as compared to controls, but pulsed light (10 and 8,000 Hz in particular) was more effective.
The two studies involving pulsed LLLT and stroke were both done by Lapchak et al. [26]. Ischemic strokes were induced in rabbits, and a pulsed laser with a wavelength of 808 nm was used. In the first study, two frequencies of pulsed light were used (100 and 1,000 Hz), both of which reduced neurological deficits more so than CW. Accordingly, pulsed LLLT may play a major role in the management of stroke patients. Lapchak et al.’s second study attempted to prove the hypothesis that LLLT’s neuroprotective effect following stroke was a result of enhanced mitochondrial energy production (increased ATP synthesis) [27]. As with the previous study, LLLT was administered following stroke induction. CW radiation raised cortical ATP levels but was unable to bring them back to baseline. PW radiation, on the other hand, not only mitigated the effects of stroke on cortical ATP levels, but was able to raise cortical ATP levels to higher than those found in healthy rabbits (those in which stroke was not induced). This study provides valuable insight into one of the potential cellular and molecular mechanisms behind the enhanced neurogenesis (and improved clinical outcomes) observed in subjects receiving transcranial LLLT following stroke.
One of the nine studies reviewed found CW and PW to be equally effective in the promotion of wound healing. This study compared the effects of a CW laser (632.8 nm) and a PW laser (904 nm) on the promotion of wound healing in rabbits. Both lasers improved tensile strength during wound healing, but did not significantly improve wound-healing rates. A combined laser (CW+PW) was also tested. All three of the laser regimens improved tensile strength to a similar extent.
As mentioned earlier, there were nine studies that compared CW and PW, only two of which found CW to be more effective. These two studies involved wound healing and nerve regeneration respectively. Al-Watban and Zhang [28] study involved rats that were inflicted with aseptic wounds. The rats were divided into three groups: a control group, those irradiated with continuous wave light, and those irradiated with pulsed light at various repetition rates (100, 200, 300, 400, and 500 Hz). Of the pulse repetition rates administered, 100 Hz was the most efficacious and 500 Hz the least. Both CW and PW (635 nm) promoted wound healing, but CW was more efficacious. These results conflict with earlier studies that found pulsed light to be more beneficial in the promotion of wound healing. However, it should be noted that the difference between CW and PW treated subjects was small (a relative wound healing rate of 4.81 as compared to 4.32).
The second study that found CW to be more effective than PW involved nerve regeneration. There were three articles involving nerve regeneration, all of which found pulsed LLLT to be ineffective, as discussed in the section below entitled “Studies Involving Nerve Conduction and Regeneration.” Of these three, only Gigo-Benato et al. [23] compared CW (808 nm) and PW (905 nm). This study involved rats in which the left median nerve was completely transected and then repaired by end-to-end neurorrhaphy. The CW laser (808 nm) promoted faster nerve and muscle recovery than the pulsed laser (905 nm). However, Gigo-Benato also tested a combination of the CW and pulsed lasers, finding this to be the most effective of all. In other words, seven of the nine studies comparing CW and PW found pulsing to play a beneficial role. Only one of the nine studies found no role of PW, and even in this study the benefit of CW over PW was minimal.
STUDIES INVOLVING THE USE OF COMBINED LASERS (CW+PW)
We reviewed three studies, as recorded in Table 2, which investigated the role of a combined laser (using both CW and PW). Of these, only Gigo-Benato’s study compared the combined laser to stand alone CW or PW. This study has been discussed in the above section: the combined laser was found to be effective in stimulating nerve regeneration, more so than CW or PW alone.
Studies Involving the Use of Combined Lasers (CW + PW)
The two other studies used a combined laser (CW and PW) to administer laser acupuncture, along with Transcutaneous Electrical Nerve Stimulation (TENS), to patients with symptoms of pain. Naeser et al. [29] administered this “triple therapy” to patients suffering from carpal tunnel syndrome (CTS). Eleven patients with mild-to-moderate symptoms of CTS were selected, all of who had failed to respond to standard medical or surgical treatment regimens. Subjects were divided into two groups, one of which received sham irradiation and the other that received a combined treatment of LLLT (CW and pulsed) and TENS. As compared to controls, the treated group experienced statistically significant improvement and remained stable for 1–3 years. The results of this study are promising, and indicate a possible role of LLLT and TENS in the conservative management of CTS.
Ceccherelli et al. [30] administered laser acupuncture to patients suffering from myofascial pain. In this double-blinded placebo controlled trial, patients received either the same “triple therapy” as in the Naeser et al. study (CW, PW, and TENS) or sham irradiation, every other day over the course of 24 days. Results were encouraging, with the treatment group experiencing a significant improvement in symptoms, both immediately after the treatment regimen and at a 3-month follow up visit.
In both preceding studies, the combined regimen of CW, PW, and TENS was compared to untreated controls, and found to be effective. However, neither study compared CW and PW or administered CW, PW, or TENS individually. As such, it is difficult to determine whether standalone CW or PW would have produced similar results, or if the combined regimen (along with TENS) was necessary.
STUDIES EVALUATING THE USE OF PULSED LASERS
Of the 33 studies reviewed, 21 of them compared PW treated subjects with untreated controls, as reported in Table 3. Of these, fourteen studies found pulsed LLLT to be effective, whereas seven of them found PW treated subjects to have no benefit over untreated controls. Only one study found PW to have a worse outcome than controls. Of the fourteen studies that found pulsed LLLT to be effective, seven involved the promotion of wound healing, four involved the attenuation of pain, two involved the promotion of bone and cartilage growth respectively, and one involved the treatment of a very rare condition (hyperphagic syndrome caused by traumatic brain injury). Of the seven studies that found no benefit to pulsed light, three involved the promotion of nerve conduction, two involved the promotion of nerve regeneration, and the remaining two involved the attenuation of pain.
If pulsed LLLT is effective (or ineffective), then what pulse repetition rates are to be used (or avoided)? Ten of the 33 articles reviewed tested and compared various repetition rates, as reported in Table 4. Four of these studies involved the use of pulsed LLLT to promote wound healing. Longo et al. [31] used the pulse repetition rates of 1,500 and 3,000 Hz, and found only the latter setting to promote wound healing. Korolev et al. [32] similarly used two pulse repetition rates, 500 and 3,000 Hz. In this case, both were found to be effective but 500 Hz was more so. Al-Watban and Zhang [28] compared five different pulse repetition rates (100, 200, 300, 400 and 500 Hz), finding 100 Hz to be the most effective and 500 Hz the least. el Sayed and Dyson [33] compared four different pulse repetition rates (2.5, 20, 292, and 20,000 Hz), and found only the two middle values (20 and 292 Hz) beneficial. The more effective pulse repetition rates in these four studies were very disparate, including 20, 100, 292, 500, and 3,000 Hz (a range of 20–3,000 Hz).
Two studies compared the role of various pulse repetition rates in the attenuation of pain. Ponnudurai et al. [34] used laser photobiostimulation to decrease pain levels in rats, and investigated the effect of using various pulsing frequencies (4, 60, and 200 Hz). The rat tail-flick test was utilized, and tail-flick latencies were measured at five intervals between 30 minutes and 7 days following irradiation. The pulsing frequency of 4 Hz increased pain threshold rapidly but very transiently, whereas 60 Hz produced a delayed but longer lasting effect. On the other hand, 200 Hz failed to produce any hypoalgesic effect whatsoever. Sushko et al. [25] conducted a similar experiment, using mice instead of rats. The center of pain was irradiated (610–910 nm) for 10 minutes with either CW or pulsed light (10, 600, and 8,000 Hz). Both modes of delivery (CW and pulsed) reduced the behavioral manifestations of somatic pain as compared to controls, but pulsed light was more effective. In particular, 10 and 8,000 Hz produced the best effect. The more effective pulse repetition rates from these two studies (involving pain attenuation) included 4, 10, 60, and 8,000 Hz (a range of 4–8,000 Hz), and the less effective pulse repetition rates included 200 and 600 Hz.
Lapchak et al. [26] not only compared CW and PW, but also pulsed light at two different repetition rates, P1 (1,000 Hz) and P2 (100 Hz). Ischemic strokes were induced in rabbits, and the neuroprotective effects of LLLT were assessed via behavioral analysis 48 hours post-stroke. Both P1 (1,000 Hz) and P2 (100 Hz) produced a similar effect (superior to CW).
Rezvani et al. [35] studied the use of low level light therapy to prevent X-ray induced late dermal necrosis. An X-ray dose of 23.4 Gy is known to invariably cause dermal necrosis after 10–16 weeks. This dose was delivered to pigs, which were then treated with LLLT for several weeks using various wavelengths (660, 820, 880, and 950 nm) pulsed at either 2.5 or 5,000 Hz. Light pulsed at 2.5 Hz did not reduce the incidence of dermal necrosis. On the other hand, light pulsed at 5,000 Hz significantly reduced (P = 0.001) the incidence to 52% when given 6–16 weeks after irradiation.
Of the 10 articles reviewed that compared various pulse repetition rates, two of them involved in vitro experiments. Brondon et al. [36] undertook a study to determine if pulsing light would overcome the filtering effects of melanin. Melanin filters were placed in front of human HEP-2 cells, which were then irradiated for 72 hours (670 nm wavelength) with either CW or pulsed light at various repetition rates (6, 18, 36, 100, and 600 Hz). Both cell proliferation and oxidative burst activity, were increased in the group treated with pulsed light, indicating that pulsed light is indeed better able to penetrate melanin rich skin. Specifically, cell proliferation was maximal at 100 Hz at 48 and 72 hours (n = 4, P≤0.05), and oxidative burst was maximal at 600 Hz (n = 4, P≤0.05).
Ueda and Shimizu [37] studied the effects of pulsed low-level light on bone formation in vitro. Osteoblast-like cells were isolated from fetal rat calvariae; one group was not irradiated at all, another was irradiated with continuous wave light, and the third group with pulsed light at three repetition rates (1, 2, and 8 Hz). As compared to the control group, both CW and PW light resulted in increased cellular proliferation, bone nodule formation, alkaline phosphatase (ALP) gene expression, and ALP activity. Pulsed light at 2 Hz stimulated these factors the most.
Out of all 10 articles that compared various pulse repetition rates, the following pulse repetition rates were found to be beneficial: 2, 10, 20, 100, 292, 500, 600, 1,000, 3,000, 5,000, and 8,000 Hz. In this wide range of frequencies (2–8,000 Hz), no particular frequencies stood out as being particularly more or less useful than others.
STUDIED INVOLVING WOUND HEALING
Ten studies out of the 33 involved LLLT’s role in the promotion of wound healing, as recorded in Table 5. Only two of these studies compared CW and PW. Kymplova et al. [24] found pulsed LLLT to promote wound healing over CW, whereas Al-Watban and Zhang [28] found CW to be slightly more effective than PW. Both studies used light of a similar wavelength (670 vs. 635 nm), although the pulse repetition rates used by Kymplova et al. were lower (10–50 Hz vs. 100–500 Hz in Al-Watban et al.’s study). The energy densities applied were also different (2 J/cm2 vs. 1 J/cm2).
Every study reviewed found pulsed LLLT effective in promoting wound healing (as compared to untreated controls), including the Al-Watban et al. study. Six of these studies used light in the wavelength range of 820–956 nm, and four in the range of 632.8–670 nm. Once again, a wide range of frequencies were used (2.5–20,000 Hz), most of which were found to promote wound healing. (Tested frequencies included 2.5, 5, 8.58, 10, 15.6, 20, 25, 31.2, 50, 78, 80, 287, 292, 500, 700, 3,000, 4,672, 9,000, and 20,000 Hz). Most of these articles also reported energy densities, usually in the range of 1–2 J/cm2.
STUDIES INVOLVING NERVE CONDUCTION AND REGENERATION
We reviewed three articles evaluating the role of pulsed LLLT in the promotion of nerve conduction, and another three involving nerve regeneration, as reported in Table 6. Unlike the studies involving wound healing where positive outcomes were reported, all six of these studies reported negative outcomes with pulsed light. Five of these studies found PW to have no statistically significant effect on outcome, whereas one of them found PW to have a deleterious effect. There was no study that directly compared CW and PW in regards to nerve conduction. Walsh et al. [38] conducted a study with 32 human volunteers to determine if pulsed LLLT would influence nerve conduction in the superficial radial nerve. Action potentials were measured pre- and post-irradiation (at 5, 10, and 15 minutes). No significant difference was appreciated between control and treatment groups, indicating that LLLT with those particular pulsing parameters and dosimetry had no specific neurophysiologic effects on nerve conduction. Bagis et al. [39] and Comelekoglu et al. [40] obtained similar negative results using frog nerves. Walsh et al. used a wavelength of 820 nm, whereas Bagis et al. used a 904 nm laser. All three studies tested pulse repetition rates within the range of 1–128 Hz.
Studies Involving Nerve Conduction and Regeneration
Similarly, the nerve regeneration studies reviewed reported negative outcomes. Chen et al. [41] found PW to have a counterproductive effect, reducing nerve regeneration as compared to untreated controls. Only one study compared CW with PW, and found the former to be superior to the latter. However, the combined laser (CW+PW) was superior to CW alone, indicating that there might in fact be a role of pulsing in nerve regeneration.
STUDIES INVOLVING PAIN ATTENUATION
Nine of the thirty-three studies involved pulsed LLLT’s role in the attenuation of pain, as reported in Table 7. Of these, only one of them directly compared CW and PW. This study was conducted by Sushko et al. [25] and found that although both CW and PW decreased pain levels, PW was more effective. This study also determined that pulse repetition rates of 10 and 8,000 Hz were more effective than 600 Hz. Ponnudurai et al. [34] similarly compared various pulse repetition rates (4, 60, and 200 Hz). A rapid but transient analgesic effect was exhibited with 4 Hz, whereas a delayed but longer lasting effect was achieved with 60 Hz. On the other hand, 200 Hz failed to produce any analgesic effect whatsoever.
Two of the studies used a combined laser (CW+PW) along with TENS; both found the combined regimen to be effective. The five remaining studies compared pulsed LLLT with untreated controls. Three of these studies found pulsed LLLT to be effective, whereas two did not. Of the nine total studies on pain attenuation, seven found pulsed LLLT to be effective in its role of attenuating pain. Only two studies found no statistically significant effect. However, it should be noted that both of these involved pain of a different nature than commonly tested in pulsed LLLT studies. The first of these was by Craig et al. [42] and involved the use of pulsed LLLT to relieve the symptoms of delayed-onset muscle soreness (DOMS). DOMS refers to the feeling of pain and muscle stiffness that can result 1–3 days after intense sporting activity such as weightlifting. This pain is duller in quality than that tested in the other studies. The second study that showed no benefit to pulsed LLLT, published by de Bie et al. [43], involved the treatment of lateral ankle sprains.
STUDIES INVOLVING ISCHEMIC STROKE
Table 8 records the two studies that involved pulsed LLLT and stroke. In the first study, PW but not CW decreased neurological deficits when delivered six hours post-stroke. Two pulse repetition rates were tested (100 and 1,000 Hz) and found to be equally effective. On the other hand, both CW and PW produced no benefit if delivered 12 hours post-stroke, indicating that timely administration of LLLT is essential.
The second study investigated the possible mechanisms behind the neuroprotective effect of LLLT. It was postulated that LLLT enhances mitochondrial energy production (and ATP synthesis), which allows for enhanced neurogenesis. This hypothesis was tested using the rabbit small clot embolic stroke model (RSCEM). Four groups of rabbits were used: (1) a naïve control group which was neither embolized or irradiated, (2) a placebo group which was embolized and sham irradiated, (3) an embolized group which was irradiated with CW (808 nm), and (4) an embolized group which was irradiated with pulsed light (808 nm) at two different frequencies. Forty-five percent less cortical ATP was measured in the second group (placebo) as compared to the first (naïve), confirming the hypothesis that ischemic strokes decrease cortical mitochondrial energy. All laser irradiated groups were able to mitigate this effect. CW radiation managed to raise the cortical ATP levels by 41%, whereas PW administration raised these levels by over 150%. Surprisingly, this was even higher than the cortical ATP content measured in naïve rabbits that had never suffered stroke.
OTHER APPLICATIONS OF PULSED MODALITIES IN BIOMEDICINE
Many of the modalities of treatment employed in biomedicine and physical therapy are used in pulsed format [44]. Electricity, electromagnetic fields and ultrasound are applied with particular pulse structures. It may be possible to gain some insight into the effect of pulsing structures in LLLT by a brief review of the other pulsed modalities. Transcutaneous electrical neural stimulation (TENS) is the application of pulses of electric current to the skin [45]. This application stimulates the brain and has been used for the treatment of various psychological and neurological conditions, including Parkinson’s, epilepsy, chronic pain, depression, and neuromuscular rehabilitation. Frequencies usually fall between 5 and 25 Hz, but may range from 2 to 80 Hz [46]. Deep brain stimulation (DBS) is a surgical treatment involving the implantation of a brain pacemaker, a medical device that sends electrical impulses to specific parts of the brain. DBS has the potential to provide substantial benefit to patients suffering from a variety of neurological conditions, including epilepsy, Parkinson’s disease, dystonia, Tourette’s syndrome, and depression [47]. The Food and Drug Administration (FDA) approved DBS at 130 Hz as a treatment for essential tremor in 1997, for Parkinson’s disease in 2002, and dystonia in 2003. Pulsed electromagnetic field (PEMF) therapy has been used for a wide range of conditions, including bone healing and regeneration [48], osteoporosis [49], arthritis [50] wound healing and pain [51], carpal tunnel syndrome [52], spinal cord injury [53], nerve regeneration [54], soft tissue injuries [55], and cancer [56]. Frequencies used for these conditions range from 1 Hz (“low”) to 200 Hz (“high”). Transcranial magnetic stimulation (TMS) is a noninvasive method used to excite neurons in the brain. Weak electric currents are induced by butterfly coils positioned above the head. TMS has been approved for the treatment of resistant depression in several countries and is under investigation for migraine [57], aphasia [58], and tinnitus [59]. Low-intensity pulsed ultrasound (LIPUS) utilizes a non-thermal mechanism of action, which can be used to promote bone healing by inducing the expression of growth factors and prostaglandins, which stimulate osteoblasts, chondrocytes and fibroblasts [60].
CONCLUSION
There has been remarkably little information available in the peer-reviewed literature on the rationale for using pulsed lasers or pulsed light in LLLT rather than CW. Moreover there is no consensus on the effects of different frequencies and pulse parameters on the physiology and therapeutic response of the various disease states that are often treated with laser therapy. This has allowed manufacturers to claim advantages of pulsing without hard evidence to back up their claims.
CW light is the gold standard and has been used for all LLLT applications. However, this review of the literature indicates that overall pulsed light may be superior to CW light with everything else being equal. This seemed to be particularly true for wound healing and post-stroke management. On the other hand, PW as a solo treatment may be less beneficial than CW in patients requiring nerve regeneration. This could possibly be explained by the mechanism of action LLLT that can either cause cell stimulation or cell inhibition or both stimulation and inhibition at the same time on different cell types. It is possible that stimulation in neurons is desired to promote neurogenesis following stroke (increased mitochondrial synthesis of ATP results in more energy for neurons to regenerate themselves), whereas inhibition of inflammatory cells, inhibition of immune response or inhibition of the glial scar may also occur at the same time. The logic in favor of PW is that cells may need periods of rest, without which they can no longer be stimulated further.
Considering that the biology of LLLT is known to be complex, it is likely that there may several optimal sets of pulse parameters and that these may relate to the specific wavelengths and chromophores and may well also be affected by other optical properties of tissues.
It was impossible to draw any meaningful correlations between pulse frequency and pathological condition, due to the wide-ranging and disparate data. As for other pulse parameters, these were in general poorly and inconsistentl
Intro: Low level light (or laser) therapy (LLLT) is a rapidly growing modality used in physical therapy, chiropractic, sports medicine and increasingly in mainstream medicine. LLLT is used to increase wound healing and tissue regeneration, to relieve pain and inflammation, to prevent tissue death, to mitigate degeneration in many neurological indications. While some agreement has emerged on the best wavelengths of light and a range of acceptable dosages to be used (irradiance and fluence), there is no agreement on whether continuous wave or pulsed light is best and on what factors govern the pulse parameters to be chosen.
Background: Low level light (or laser) therapy (LLLT) is a rapidly growing modality used in physical therapy, chiropractic, sports medicine and increasingly in mainstream medicine. LLLT is used to increase wound healing and tissue regeneration, to relieve pain and inflammation, to prevent tissue death, to mitigate degeneration in many neurological indications. While some agreement has emerged on the best wavelengths of light and a range of acceptable dosages to be used (irradiance and fluence), there is no agreement on whether continuous wave or pulsed light is best and on what factors govern the pulse parameters to be chosen.
Abstract: Abstract
BACKGROUND AND OBJECTIVE:
Low level light (or laser) therapy (LLLT) is a rapidly growing modality used in physical therapy, chiropractic, sports medicine and increasingly in mainstream medicine. LLLT is used to increase wound healing and tissue regeneration, to relieve pain and inflammation, to prevent tissue death, to mitigate degeneration in many neurological indications. While some agreement has emerged on the best wavelengths of light and a range of acceptable dosages to be used (irradiance and fluence), there is no agreement on whether continuous wave or pulsed light is best and on what factors govern the pulse parameters to be chosen.
STUDY DESIGN/MATERIALS AND METHODS:
The published peer-reviewed literature was reviewed between 1970 and 2010.
RESULTS:
The basic molecular and cellular mechanisms of LLLT are discussed. The type of pulsed light sources available and the parameters that govern their pulse structure are outlined. Studies that have compared continuous wave and pulsed light in both animals and patients are reviewed. Frequencies used in other pulsed modalities used in physical therapy and biomedicine are compared to those used in LLLT.
CONCLUSION:
There is some evidence that pulsed light does have effects that are different from those of continuous wave light. However further work is needed to define these effects for different disease conditions and pulse structures.
(c) 2010 Wiley-Liss, Inc.
Methods: The published peer-reviewed literature was reviewed between 1970 and 2010.
Results: The basic molecular and cellular mechanisms of LLLT are discussed. The type of pulsed light sources available and the parameters that govern their pulse structure are outlined. Studies that have compared continuous wave and pulsed light in both animals and patients are reviewed. Frequencies used in other pulsed modalities used in physical therapy and biomedicine are compared to those used in LLLT.
Conclusions: There is some evidence that pulsed light does have effects that are different from those of continuous wave light. However further work is needed to define these effects for different disease conditions and pulse structures.
Shining light on the head: Photobiomodulation for brain disorders
Michael R. Hamblin - 10.1016/j.bbacli.2016.09.002 (Publication) 4466 This is 27 pages of independent analysis of how photobiomodulation effects the brain. Covers wavelengths, dosage, pulsing, depths and underlying reactions. Amazing.
Photobiomodulation (PBM) describes the use of red or near-infrared light to stimulate, heal, regenerate, and protect tissue that has either been injured, is degenerating, or else is at risk of dying. One of the organ systems of the human body that is most necessary to life, and whose optimum functioning is most worried about by humankind in general, is the brain. The brain suffers from many different disorders that can be classified into three broad groupings: traumatic events (stroke, traumatic brain injury, and global ischemia), degenerative diseases (dementia, Alzheimer's and Parkinson's), and psychiatric disorders (depression, anxiety, post traumatic stress disorder). There is some evidence that all these seemingly diverse conditions can be beneficially affected by applying light to the head. There is even the possibility that PBM could be used for cognitive enhancement in normal healthy people. In this transcranial PBM (tPBM) application, near-infrared (NIR) light is often applied to the forehead because of the better penetration (no hair, longer wavelength). Some workers have used lasers, but recently the introduction of inexpensive light emitting diode (LED) arrays has allowed the development of light emitting helmets or “brain caps”. This review will cover the mechanisms of action of photobiomodulation to the brain, and summarize some of the key pre-clinical studies and clinical trials that have been undertaken for diverse brain disorders.
Photobiomodulation (PBM) as it is known today (the beneficial health benefits of light therapy had been known for some time before), was accidently discovered in 1967, when Endre Mester from Hungary attempted to repeat an experiment recently published by McGuff in Boston, USA [1]. McGuff had used a beam from the recently discovered ruby laser [2], to destroy a cancerous tumor that had been experimentally implanted into a laboratory rat. However (unbeknownst to Mester) the ruby laser that had been built for him, was only a tiny fraction of the power of the laser that had previously been used by McGuff. However, instead of curing the experimental tumors with his low-powered laser, Mester succeeded in stimulating hair regrowth and wound healing in the rats, in the sites where the tumors had been implanted [3], [4]. This discovery led to a series of papers describing what Mester called “laser biostimulation”, and soon became known as “low level laser therapy” (LLLT) [5], [6], [7].
LLLT was initially primarily studied for stimulation of wound healing, and reduction of pain and inflammation in various orthopedic conditions such as tendonitis, neck pain, and carpal tunnel syndrome [8]. The advent of light emitting diodes (LED) led to LLLT being renamed as “low level light therapy”, as it became more accepted that the use of coherent lasers was not absolutely necessary, and a second renaming occurred recently [9] when the term PBM was adopted due to uncertainties in the exact meaning of “low level”.
The most well studied mechanism of action of PBM centers around cytochrome c oxidase (CCO), which is unit four of the mitochondrial respiratory chain, responsible for the final reduction of oxygen to water using the electrons generated from glucose metabolism [10]. The theory is that CCO enzyme activity may be inhibited by nitric oxide (NO) (especially in hypoxic or damaged cells). This inhibitory NO can be dissociated by photons of light that are absorbed by CCO (which contains two heme and two copper centers with different absorption spectra) [11]. These absorption peaks are mainly in the red (600–700 nm) and near-infrared (760–940 nm) spectral regions. When NO is dissociated, the mitochondrial membrane potential is increased, more oxygen is consumed, more glucose is metabolized and more ATP is produced by the mitochondria.
It has been shown that there is a brief increase in reactive oxygen species (ROS) produced in the mitochondria when they absorb the photons delivered during PBM. The idea is that this burst of ROS may trigger some mitochondrial signaling pathways leading to cytoprotective, anti-oxidant and anti-apoptotic effects in the cells [12]. The NO that is released by photodissociation acts as a vasodilator as well as a dilator of lymphatic flow. Moreover NO is also a potent signaling molecule and can activate a number of beneficial cellular pathways [13]. Fig. 2 illustrates these mechanisms.
Tissue specific processes that occur after PBM and benefit a range of brain disorders. BDNF, brain-derived neurotrophic factor; LLLT, low level light therapy; NGF, nerve growth factor; NT-3, neurotrophin 3; PBM, photobiomodulation; SOD, superoxide dismutase. ...
2.3. Light sensitive ion channels and calcium
It is quite clear that there must be some other type of photoacceptor, in addition to CCO, as is clearly demonstrated by the fact that wavelengths substantially longer than the red/NIR wavelengths discussed above, can also produce beneficial effects is some biological scenarios. Wavelengths such as 980 nm [14], [15], 1064 nm laser [16], and 1072 nm LED [17], and even broad band IR light [18] have all been reported to carry out PBM type effects. Although the photoacceptor for these wavelengths has by no means been conclusively identified, the leading hypothesis is that it is primarily water (perhaps nanostructured water) located in heat or light sensitive ion channels. Clear changes in intracellular calcium can be observed, that could be explained by light-mediated opening of calcium ion channels, such as members of the transient receptor potential (TRP) super-family [19]. TRP describes a large family of ion channels typified by TRPV1, recently identified as the biological receptor for capsaicin (the active ingredient in hot chili peppers) [20]. The biological roles of TRP channels are multifarious, but many TRP channels are involved in heat sensing and thermoregulation [21].
2.4. Signaling mediators and activation of transcription factors
Most authors suggest that the beneficial effects of tPBM on the brain can be explained by increases in cerebral blood flow, greater oxygen availability and oxygen consumption, improved ATP production and mitochondrial activity [22], [23], [24]. However there are many reports that a brief exposure to light (especially in the case of experimental animals that have suffered some kind of acute injury or traumatic insult) can have effects lasting days, weeks or even months [25]. This long-lasting effect of light can only be explained by activation of signaling pathways and transcription factors that cause changes in protein expression that last for some considerable time. The effects of PBM on stimulating mitochondrial activity and blood flow is of itself, unlikely to explain long-lasting effects. A recent review listed no less than fourteen different transcription factors and signaling mediators, that have been reported to be activated after light exposure [10].
Fig. 1 illustrates two of the most important molecular photoreceptors or chromophores (cytochrome c oxidase and heat-gated ion channels) inside neuronal cells that absorb photons that penetrate into the brain. The signaling pathways and activation of transcription factors lead to the eventual effects of PBM in the brain.
Molecular and intracellular mechanisms of transcranial low level laser (light) or photobiomodulation. AP1, activator protein 1; ATP, adenosine triphosphate; Ca2 +, calcium ions; cAMP, cyclic adenosine monophosphate; NF-kB, nuclear factor kappa ...
Fig. 2 illustrates some more tissue specific mechanisms that lead on from the initial photon absorption effects explained in Fig. 1. A wide variety of processes can occur that can benefit a correspondingly wide range of brain disorders. These processes can be divided into short-term stimulation (ATP, blood flow, lymphatic flow, cerebral oxygenation, less edema). Another group of processes center around neuroprotection (upregulation of anti-apoptotic proteins, less excitotoxity, more antioxidants, less inflammation). Finally a group of processes that can be grouped under “help the brain to repair itself” (neurotrophins, neurogenesis and synaptogenesis).
2.5. Biphasic dose response and effect of coherence
The biphasic dose response (otherwise known as hormesis, and reviewed extensively by Calabrese et al. [26]) is a fundamental biological law describing how different biological systems can be activated or stimulated by low doses of any physical insult or chemical substance, no matter how toxic or damaging this insult may be in large doses. The most well studied example of hormesis is that of ionizing radiation, where protective mechanisms are induced by very low exposures, that can not only protect against subsequent large doses of ionizing radiation, but can even have beneficial effects against diseases such as cancer using whole body irradiation [27].
There are many reports of PBM following a biphasic dose response (sometimes called obeying the Arndt-Schulz curve [28], [29]. A low dose of light is beneficial, but raising the dose produces progressively less benefit until eventually a damaging effect can be produced at very high light [30]. It is often said in this context that “more does not mean more”.
Another question that arises in the field of PBM is whether the coherent monochromatic lasers that were used in the original discovery of the effect, and whose use continued for many years, are superior to the rather recent introduction of LEDs, that are non-coherent and have a wider band-spread (generally 30 nm full-width half-maximum). Although there are one or two authors who continue to believe that coherent lasers are superior [31], most commentators feel that other parameters such as wavelength, power density, energy density and total energy are the most important determinants of efficacy [8].
3. Tissue optics, direct versus systemic effects, light sources
3.1. Light penetration into the brain
Due to the growing interest in PBM of the brain, several tissue optics laboratories have investigated the penetration of light of different wavelengths through the scalp and the skull, and to what depths into the brain this light can penetrate. This is an intriguing question to consider, because at present it is unclear exactly what threshold of power density in mW/cm2 is required in the b5rain to have a biological effect. There clearly must be a minimum value below which the light can be delivered for an infinite time without doing anything, but whether this is in the region of μW/cm2 or mW/cm2 is unknown at present.
Functional near-infrared spectroscopy (fNIRS) using 700–900 nm light has been established as a brain imaging technique that can be compared to functional magnetic resonance imaging (fMRI) [32]. Haeussinger et al. estimated that the mean penetration depth (5% remaining intensity) of NIR light through the scalp and skull was 23:6 + 0:7 mm [33]. Other studies have found comparable results with variations depending on the precise location on the head and wavelength [34], [35].
Jagdeo et al. [36] used human cadaver heads (skull with intact soft tissue) to measure penetration of 830 nm light, and found that penetration depended on the anatomical region of the skull (0.9% at the temporal region, 2.1% at the frontal region, and 11.7% at the occipital region). Red light (633 nm) hardly penetrated at all. Tedord et al. [37] also used human cadaver heads to compare penetration of 660 nm, 808 nm, and 940 nm light. They found that 808 nm light was best and could reach a depth in the brain of 40–50 mm. Lapchak et al. compared the transmission of 810 nm light through the skulls of four different species, and found mouse transmitted 40%, while for rat it was 21%, rabbit it was 11.3 and for human skulls it was only 4.2% [38]. Pitzschke and colleagues compared penetration of 670 nm and 810 nm light into the brain when delivered by a transcranial or a transphenoidal approach, and found that the best combination was 810 nm delivered transphenoidally [39]. In a subsequent study these authors compared the effects of storage and processing (frozen or formalin-fixed) on the tissue optical properties of rabbit heads [40]. Yaroslavsky et al. examined light penetration of different wavelengths through different parts of the brain tissue (white brain matter, gray brain matter, cerebellum, and brainstem tissues, pons, thalamus). Best penetration was found with wavelengths between 1000 and 1100 nm [41].
Henderson and Morries found that between 0.45% and 2.90% of 810 nm or 980 nm light penetrated through 3 cm of scalp, skull and brain tissue in ex vivo lamb heads [42].
3.2. Systemic effects
It is in fact very likely that the beneficial effects of PBM on the brain cannot be entirely explained by penetration of photons through the scalp and skull into the brain itself. There have been some studies that have explicitly addressed this exact issue. In a study of PBM for Parkinson's disease in a mouse model [43]. Mitrofanis and colleagues compared delivering light to the mouse head, and also covered up the head with aluminum foil so that they delivered light to the remainder of the mouse body. They found that there was a highly beneficial effect on neurocognitive behavior with irradiation to the head, but nevertheless there was also a statistically significant (although less pronounced benefit, referred to by these authors as an ‘abscopal effect”) when the head was shielded from light [44]. Moreover Oron and co-workers [45] have shown that delivering NIR light to the mouse tibia (using either surface illumination or a fiber optic) resulted in improvement in a transgenic mouse model of Alzheimer's disease (AD). Light was delivered weekly for 2 months, starting at 4 months of age (progressive stage of AD). They showed improved cognitive capacity and spatial learning, as compared to sham-treated AD mice. They proposed that the mechanism of this effect was to stimulate c-kit-positive mesenchymal stem cells (MSCs) in autologous bone marrow (BM) to enhance the capacity of MSCs to infiltrate the brain, and clear β-amyloid plaques [46]. It should be noted that the calvarial bone marrow of the skull contains substantial numbers of stem cells [47].
3.3. Laser acupuncture
Laser acupuncture is often used as an alternative or as an addition to traditional Chinese acupuncture using needles [48]. Many of the applications of laser acupuncture have been for conditions that affect the brain [49] such as Alzheimer's disease [50] and autism [51] that have all been investigated in animal models. Moreover laser acupuncture has been tested clinically [52].
3.4. Light sources
A wide array of different light sources (lasers and LEDs) have been employed for tPBM. One of the most controversial questions which remains to be conclusively settled, is whether a coherent monochromatic laser is superior to non-coherent LEDs typically having a 30 nm band-pass (full width half maximum). Although wavelengths in the NIR region (800–1100 nm) have been the most often used, red wavelengths have sometimes been used either alone, or in combination with NIR. Power levels have also varied markedly from Class IV lasers with total power outputs in the region of 10 W [53], to lasers with more modest power levels (circa 1 W). LEDs can also have widely varying total power levels depending on the size of the array and the number and power of the individual diodes. Power densities can also vary quite substantially from the Photothera laser [54] and other class IV lasers , which required active cooling (~ 700 mW/cm2) to LEDs in the region of 10–30 mW/cm2.
3.5. Usefulness of animal models when testing tPBM for brain disorders
One question that is always asked in biomedical research, is how closely do the laboratory models of disease (which are usually mice or rats) mimic the human disease for which new treatments are being sought? This is no less critical a question when the areas being studied include brain disorders and neurology. There now exist a plethora of transgenic mouse models of neurological disease [55], [56]. However in the present case, where the proposed treatment is almost completely free of any safety concerns, or any reported adverse side effects, it can be validly questioned as to why the use of laboratory animal models should be encouraged. Animal models undoubtedly have disadvantages such as failure to replicate all the biological pathways found in human disease, difficulty in accurately measuring varied forms of cognitive performance, small size of mice and rats compared to humans, short lifespan affecting the development of age related diseases, and lack of lifestyle factors that adversely affect human diseases. Nevertheless, small animal models are less expensive, and require much less time and effort to obtain results than human clinical trials, so it is likely they will continue to be used to test tPBM for the foreseeable future.
Perhaps the most well-investigated application of PBM to the brain, lies in its possible use as a treatment for acute stroke [57]. Animal models such as rats and rabbits, were first used as laboratory models, and these animals had experimental strokes induced by a variety of methods and were then treated with light (usually 810 nm laser) within 24 h of stroke onset [58]. In these studies intervention by tLLLT within 24 h had meaningful beneficial effects. For the rat models, stroke was induced by middle cerebral artery occlusion (MCAO) via an insertion of a filament into the carotid artery or via craniotomy [59], [60]. Stroke induction in the “rabbit small clot embolic model” (RSCEM) was by injection of a preparation of small blood clots (made from blood taken from a second donor rabbit) into a catheter placed in the right internal carotid artery [61]. These studies and the treatments and results are listed in Table 1.
Treatment of acute stroke was addressed in a series of three clinical trials called “Neurothera Effectiveness and Safety Trials” (NEST-1 [65], NEST-2 [66], and NEST-3 [67]) using an 810 nm laser applied to the shaved head within 24 h of patients suffering an ischemic stroke. The first study, NEST-1, enrolled 120 patients between the ages of 40 to 85 years of age with a diagnosis of ischemic stroke involving a neurological deficit that could be measured. The purpose of this first clinical trial was to demonstrate the safety and effectiveness of laser therapy for stroke within 24 h [65]. tPBM significantly improved outcome in human stroke patients, when applied at ~ 18 h post-stroke, over the entire surface of the head (20 points in the 10/20 EEG system) regardless of stroke [65]. Only one laser treatment was administered, and 5 days later, there was significantly greater improvement in the Real- but not in the Sham-treated group (p < 0.05, NIH Stroke Severity Scale). This significantly greater improvement was still present at 90 days post-stroke, where 70% of the patients treated with Real-LLLT had a successful outcome, while only 51% of Sham-controls did. The second clinical trial, NEST-2, enrolled 660 patients, aged 40 to 90, who were randomly assigned to one of two groups (331 to LLLT, 327 to sham) [68]. Beneficial results (p < 0.04) were found for the moderate and moderate-severe (but not for the severe) stroke patients, who received the Real laser protocol [68]. These results suggested that the overall severity of the individual stroke should be taken into consideration in future studies, and very severe patients are unlikely to recover with any kind of treatment. The last clinical trial, NEST-3, was planned for 1000 patients enrolled. Patients in this study were not to receive tissue plasminogen activator, but the study was prematurely terminated by the DSMB for futility (an expected lack of statistical significance) [67]. NEST-1 was considered successful, even though as a phase 1 trial, it was not designed to show efficacy. NEST-2 was partially successful when the patients were stratified, to exclude very severe strokes or strokes deep within the brain [66]. There has been considerable discussion in the scientific literature on precisely why the NEST-3 trial failed [69]. Many commentators have wondered how could tPBM work so well in the first trial, in a sub-group in the second trial, and fail in the third trial. Lapchak's opinion is that the much thicker skull of humans compared to that of the other animals discussed above (mouse, rat and rabbit), meant that therapeutically effective amounts of light were unlikely to reach the brain [69]. Moreover the time between the occurrence of a stroke and initiation of the PBMT may be an important factor. There are reports in the literature that neuroprotection must be administered as soon as possible after a stroke [70], [71]. Furthermore, stroke trials in particular should adhere to the RIGOR (rigorous research) guidelines and STAIR (stroke therapy academic industry roundtable) criteria [72]. Other contributory causes to the failure of NEST-3 may have been included the decision to use only one single tPBM treatment, instead of a series of treatments. Moreover, the optimum brain areas to be treated in acute stroke remain to be determined. It is possible that certain areas of the brain that have sustained ischemic damage should be preferentially illuminated and not others.
4.3. Chronic stroke
Somewhat surprisingly, there have not as yet been many trials of PBM for rehabilitation of stroke patients with only the occasional report to date. Naeser reported in an abstract the use of tPBM to treat chronic aphasia in post-stroke patients [73]. Boonswang et al. [74] reported a single patient case in which PBM was used in conjunction with physical therapy to rehabilitate chronic stroke damage. However the findings that PBM can stimulate synaptogenesis in mice with TBI, does suggest that tPBM may have particular benefits in rehabilitation of stroke patients. Norman Doidge, in Toronto, Canada has described the use of PBM as a component of a neuroplasticity approach to rehabilitate chronic stroke patients [75].
There have been a number of studies looking at the effects of PBM in animal models of TBI. Oron's group was the first [76] to demonstrate that a single exposure of the mouse head to a NIR laser (808 nm) a few hours after creation of a TBI lesion could improve neurological performance and reduce the size of the brain lesion. A weight-drop device was used to induce a closed-head injury in the mice. An 808 nm diode laser with two energy densities (1.2–2.4 J/cm2 over 2 min of irradiation with 10 and 20 mW/cm2) was delivered to the head 4 h after TBI was induced. Neurobehavioral function was assessed by the neurological severity score (NSS). There were no significant difference in NSS between the power densities (10 vs 20 mW/cm2) or significant differentiation between the control and laser treated group at early time points (24 and 48 h) post TBI. However, there was a significant improvement (27% lower NSS score) in the PBM group at times of 5 days to 4 weeks. The laser treated group also showed a smaller loss of cortical tissue than the sham group [76].
Hamblin's laboratory then went on (in a series of papers [76]) to show that 810 nm laser (and 660 nm laser) could benefit experimental TBI both in a closed head weight drop model [77], and also in controlled cortical impact model in mice [25]. Wu et al. [77] explored the effect that varying the laser wavelengths of LLLT had on closed-head TBI in mice. Mice were randomly assigned to LLLT treated group or to sham group as a control. Closed-head injury (CHI) was induced via a weight drop apparatus. To analyze the severity of the TBI, the neurological severity score (NSS) was measured and recorded. The injured mice were then treated with varying wavelengths of laser (665, 730, 810 or 980 nm) at an energy level of 36 J/cm2 at 4 h directed onto the scalp. The 665 nm and 810 nm groups showed significant improvement in NSS when compared to the control group at day 5 to day 28. Results are shown in Fig. 3. Conversely, the 730 and 980 nm groups did not show a significant improvement in NSS and these wavelengths did not produce similar beneficial effects as in the 665 nm and 810 nm LLLT groups [77]. The tissue chromophore cytochrome c oxidase (CCO) is proposed to be responsible for the underlying mechanism that produces the many PBM effects that are the byproduct of LLLT. COO has absorption bands around 665 nm and 810 nm while it has low absorption bands at the wavelength of 730 nm [78]. It should be noted that this particular study found that the 980 nm did not produce the same positive effects as the 665 nm and 810 nm wavelengths did; nevertheless previous studies did find that the 980 nm wavelength was an active one for LLLT. Wu et al. proposed that these dissimilar results may be due to the variance in the energy level, irradiance, etc. between the other studies and this particular study [77].
tPBM for TBI in a mouse model. Mice received a closed head injury and 4 hours later a single exposure of the head to one of four different lasers (36 J/cm2 delivered at 150 mW/cm2 over 4 min with spot size 1-cm diameter) ...
Ando et al. [25] used the 810 nm wavelength laser parameters from the previous study and varied the pulse modes of the laser in a mouse model of TBI. These modes consisted of either pulsed wave at 10 Hz or at 100 Hz (50% duty cycle) or continuous wave laser. For the mice, TBI was induced with a controlled cortical impact device via open craniotomy. A single treatment with an 810 nm Ga-Al-As diode laser with a power density of 50 mW/m2 and an energy density of 36 J/cm2 was given via tLLLT to the closed head in mice for a duration of 12 min at 4 h post CCI. At 48 h to 28 days post TBI, all laser treated groups had significant decreases in the measured neurological severity score (NSS) when compared to the control (Fig. 4A). Although all laser treated groups had similar NSS improvement rates up to day 7, the PW 10 Hz group began to show greater improvement beyond this point as seen in Fig. 4. At day 28, the forced swim test for depression and anxiety was used and showed a significant decrease in the immobility time for the PW 10 Hz group. In the tail suspension test which measures depression and anxiety, there was also a significant decrease in the immobility time at day 28, and this time also at day 1, in the PW 10 Hz group.
tPBM for controlled cortical impact TBI in a mouse model. (A) Mice received a single exposure (810 nm laser, 36 J/cm2 delivered at 50 mW/cm2 over 12 min) [121]. (B) Mice received 3 daily exposures starting 4 h post-TBI ...
Studies using immunofluorescence of mouse brains showed that tPBM increased neuroprogenitor cells in the dentate gyrus (DG) and subventricular zone at 7 days after the treatment [79]. The neurotrophin called brain derived neurotrophic factor (BDNF) was also increased in the DG and SVZ at 7 days , while the marker (synapsin-1) for synaptogenesis and neuroplasticity was increased in the cortex at 28 days but not in the DG, SVZ or at 7 days [80] (Fig. 4B). Learning and memory as measured by the Morris water maze was also improved by tPBM [81]. Whalen's laboratory [82] and Whelan's laboratory [83] also successfully demonstrated therapeutic benefits of tPBM for TBI in mice and rats respectively.
Zhang et al. [84] showed that secondary brain injury occurred to a worse degree in mice that had been genetically engineered to lack “Immediate Early Response” gene X-1 (IEX-1) when exposed to a gentle head impact (this injury is thought to closely resemble mild TBI in humans). Exposing IEX-1 knockout mice to LLLT 4 h post injury, suppressed proinflammatory cytokine expression of interleukin (IL)-Iβ and IL-6, but upregulated TNF-α. The lack of IEX-1 decreased ATP production, but exposing the injured brain to LLLT elevated ATP production back to near normal levels.
Dong et al. [85] even further improved the beneficial effects of PBM on TBI in mice, by combining the treatment with metabolic substrates such as pyruvate and/or lactate. The goal was to even further improve mitochondrial function. This combinatorial treatment was able to reverse memory and learning deficits in TBI mice back to normal levels, as well as leaving the hippocampal region completely protected from tissue loss; a stark contrast to that found in control TBI mice that exhibited severe tissue loss from secondary brain injury.
5.2. TBI in humans
Margaret Naeser and collaborators have tested PBM in human subjects who had suffered TBI in the past [86]. Many sufferers from severe or even moderate TBI, have very long lasting and even life-changing sequelae (headaches, cognitive impairment, and difficulty sleeping) that prevent them working or living any kind or normal life. These individuals may have been high achievers before the accident that caused damage to their brain [87]. Initially Naeser published a report [88] describing two cases she treated with PBM applied to the forehead twice a week. A 500 mW continuous wave LED source (mixture of 660 nm red and 830 nm NIR LEDs) with a power density of 22.2 mW/cm2 (area of 22.48 cm2), was applied to the forehead for a typical duration of 10 min (13.3 J/cm2). In the first case study the patient reported that she could concentrate on tasks for a longer period of time (the time able to work at a computer increased from 30 min to 3 h). She had a better ability to remember what she read, decreased sensitivity when receiving haircuts in the spots where LLLT was applied, and improved mathematical skills after undergoing LLLT. The second patient had statistically significant improvements compared to prior neuropsychological tests after 9 months of treatment. The patient had a 2 standard deviation (SD) increase on tests of inhibition and inhibition accuracy (9th percentile to 63rd percentile on the Stroop test for executive function and a 1 SD increase on the Wechsler Memory scale test for the logical memory test (83rd percentile to 99th percentile) [89].
Naeser et al. then went on to report a case series of a further eleven patients [90]. This was an open protocol study that examined whether scalp application of red and near infrared (NIR) light could improve cognition in patients with chronic, mild traumatic brain injury (mTBI). This study had 11 participants ranging in age from 26 to 62 (6 males, 5 females) who suffered from persistent cognitive dysfunction after mTBI. The participants' injuries were caused by motor vehicle accidents, sports related events and for one participant, an improvised explosive device (IED) blast. tLLLT consisted of 18 sessions (Monday, Wednesday, and Friday for 6 weeks) and commenced anywhere from 10 months to 8 years post-TBI. A total of 11 LED clusters (5.25 cm in diameter, 500 mW, 22.2 mW/cm2, 13 J/cm2) were applied for about 10 min per session (5 or 6 LED placements per set, Set A and then Set B, in each session). Neuropsychological testing was performed pre-LED application and 1 week, 1 month and 2 months after the final treatment. Naeser and colleagues found that there was a significant positive linear trend observed for the Stroop Test for executive function, in trial 2 inhibition (p = 0.004); Stroop, trial 4 inhibition switching (p = 0.003); California Verbal Learning Test (CVLT)-II, total trials 1–5 (p = 0.003); CVLT-II, long delay free recall (p = 0.006). Improved sleep and fewer post-traumatic stress disorder (PTSD) symptoms, if present beforehand, were observed after treatment. Participants and family members also reported better social function and a better ability to perform interpersonal and occupational activities. Although these results were significant, further placebo-controlled studies will be needed to ensure the reliability of this these data [90].
Henderson and Morries [91] used a high-power NIR laser (10–15 W at 810 and 980 nm) applied to the head to treat a patient with moderate TBI. The patient received 20 NIR applications over a 2-month period. They carried out anatomical magnetic resonance imaging (MRI) and perfusion single-photon emission computed tomography (SPECT). The patient showed decreased depression, anxiety, headache, and insomnia, whereas cognition and quality of life improved, accompanied by changes in the SPECT imaging.
There was a convincing study [92] carried out in an AβPP transgenic mouse of AD. tPBM (810 nm laser) was administered at different doses 3 times/week for 6 months starting at 3 months of age. The numbers of Aβ plaques were significantly reduced in the brain with administration of tPBM in a dose-dependent fashion. tPBM mitigated the behavioral effects seen with advanced amyloid deposition and reduced the expression of inflammatory markers in the transgenic mice. In addition, TLT showed an increase in ATP levels, mitochondrial function, and c-fos expression suggesting that there was an overall improvement in neurological function.
6.2. Humans
There has been a group of investigators in Northern England who have used a helmet built with 1072 nm LEDs to treat AD, but somewhat surprisingly no peer-reviewed publications have described this approach [93]. However a small pilot study (19 patients) that took the form of a randomized placebo-controlled trial investigated the effect of the Vielight Neuro system (see Fig. 5A) (a combination of tPBM and intranasal PBM) on patients with dementia and mild cognitive impairment [94]. This was a controlled single blind pilot study in humans to investigate the effects of PBM on memory and cognition. 19 participants with impaired memory/cognition were randomized into active and sham treatments over 12 weeks with a 4-week no-treatment follow-up period. They were assessed with MMSE and ADAS-cog scales. The protocol involved in-clinic use of a combined transcranial-intranasal PBM device; and at-home use of an intranasal-only PBM device and participants/ caregivers noted daily experiences in a journal. Active participants with moderate to severe impairment (MMSE scores 5–24) showed significant improvements (5-points MMSE score) after 12 weeks. There was also a significant improvement in ADAS-cog scores (see Fig. 5B). They also reported better sleep, fewer angry outbursts and decreased anxiety and wandering. Declines were noted during the 4-week no-treatment follow-up period. Participants with mild impairment to normal (MMSE scores of 25 to 30) in both the active and sham sub-groups showed improvements. No related adverse events were reported.
tPBM for Alzheimer's disease. (A) Nineteen patients were randomized to receive real or sham tPBM (810 nm LED, 24.6 J/cm2 at 41 mW/cm2). (B) Significant decline in ADAS-cog (improved cognitive performance) in real but not sham (unpublished ...
An interesting paper from Russia [95] described the use of intravascular PBM to treat 89 patients with AD who received PBM (46 patients) or standard treatment with memantine and rivastigmine (43 patients). The PBM consisted of threading a fiber-optic through a cathéter in the fémoral artery and advancing it to the distal site of the anterior and middle cerebral arteries and delivering 20 mW of red laser for 20–40 min. The PBM group had improvement in cerebral microcirculation leading to permanent (from 1 to 7 years) reduction in dementia and cognitive recovery.
The majority of studies on PBM for Parkinson's disease have been in animal models and have come from the laboratory of John Mitrofanis in Australia [96]. Two basic models of Parkinson's disease were used. The first employed administration of the small molecule (MPTP or 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) to mice [97]. MPTP was discovered as an impurity in an illegal recreational drug to cause Parkinson's like symptoms (loss of substantia nigra cells) in young people who had taken this drug [98]. Mice were treated with tPBM (670-nm LED, 40 mW/cm2, 3.6 J/cm2) 15 min after each MPTP injection repeated 4 times over 30 h. There were significantly more (35%–45%) dopaminergic cells in the brains of the tPBM treated mice [97]. A subsequent study showed similar results in a chronic mouse model of MPTP-induced Parkinson's disease [99]. They repeated their studies in another mouse model of Parkinson's disease, the tau transgenic mouse strain (K3) that has a progressive degeneration of dopaminergic cells in the substantia nigra pars compacta (SNc) [100]. They went on to test a surgically implanted intracranial fiber designed to deliver either 670 nm LED (0.16 mW) or 670 nm laser (67 mW) into the lateral ventricle of the brain in MPTP-treated mice [101]. Both low power LED and high power laser were effective in preserving SNc cells, but the laser was considered to be unsuitable for long-term use (6 days) due to excessive heat production. As mentioned above, these authors also reported a protective effect of abscopal light exposure (head shielded) in this mouse model [43]. Recently this group has tested their implanted fiber approach in a model of Parkinson's disease in adult Macaque monkeys treated with MPTP [102]. Clinical evaluation of Parkinson's symptoms (posture, general activity, bradykinesia, and facial expression) in the monkeys were improved at low doses of light (24 J or 35 J) compared to high doses (125 J) [103].
The only clinical report of PBM for Parkinson's disease in humans was an abstract presented in 2010 [104]
Role of low-level laser therapy in neurorehabilitation.
Hashmi JT1, Huang YY, Osmani BZ, Sharma SK, Naeser MA, Hamblin MR. - PM R. 2010 Dec;2(12 Suppl 2):S292-305. doi: 10.1016/j.pmrj.2010.10.013. (Publication) 1764 This summary publication goes into depth the mechanisms involved in LLLT with detailed sections on stroke, TBI and degenerative nervous system disease.
This year marks the 50th anniversary of the discovery of the laser. The development of lasers for medical use, which became known as low-level laser therapy (LLLT) or photobiomodulation, followed in 1967. In recent years, LLLT has become an increasingly mainstream modality, especially in the areas of physical medicine and rehabilitation. At first used mainly for wound healing and pain relief, the medical applications of LLLT have broadened to include diseases such as stroke, myocardial infarction, and degenerative or traumatic brain disorders. This review will cover the mechanisms of LLLT that operate both on a cellular and a tissue level. Mitochondria are thought to be the principal photoreceptors, and increased adenosine triphosphate, reactive oxygen species, intracellular calcium, and release of nitric oxide are the initial events. Activation of transcription factors then leads to expression of many protective, anti-apoptotic, anti-oxidant, and pro-proliferation gene products. Animal studies and human clinical trials of LLLT for indications with relevance to neurology, such as stroke, traumatic brain injury, degenerative brain disease, spinal cord injury, and peripheral nerve regeneration, will be covered.
INTRODUCTION
It was not long after the discovery of the first lasers (the ruby laser in 1960 and the helium-neon [HeNe] laser in 1961) that they began to be used in medical applications. In 1967, Endre Mester in Hungary noticed the ability of the HeNe laser to increase hair growth [1] and stimulate wound healing in mice [2], and, shortly afterward, he began to use lasers to treat patients with nonhealing skin ulcers [3]. Since those early days, the use of low-power lasers (as opposed to high-power lasers that can destroy tissue by a photothermal effect) has steadily increased in diverse areas of medical practice that require healing, prevention of tissue death, pain relief, reduction of inflammation, and regenerative medicine. Some of the different organ systems, diseases, and injuries that have been effectively treated with low-level laser therapy (LLLT) are schematically shown in Figure 1.
Diagram of the various medical applications of low-level light therapy.
Nevertheless, this modality, which is variously known as LLLT or photobiomodulation, remains controversial. The reasons for this lack of general acceptance among both the medical community and the general public at large are 2-fold. First, widespread uncertainty and confusion exists about the mechanisms of action of LLLT at the molecular, cellular, and tissue levels. Second, a large number of parameters (eg, wavelength, fluence, irradiance, treatment timing and repetition, pulsing, and polarization) can be chosen in designing LLLT protocols. Furthermore, a biphasic dose response exists in laser therapy [4], which describes the observation that increasing the overall “dose” of the laser either by increasing the power density or by increasing the illumination time may have a counter-productive effect compared with the benefit obtained with lower doses. Taken together, these considerations may explain why a number of negative studies have been published; however, this should not be taken to imply that LLLT in general does not work but rather that the laser parameters used in those particular studies were ineffective.
In recent years, the development of light-emitting diodes (LEDs) as alternative light sources for LLLT has added to the confusion. These devices produce light with wavelengths similar to those of lasers, but they have broader output peaks (ie, they are less monochromatic) and lack the coherence that is a particular feature of laser light. LEDs have the advantage of being significantly less expensive than laser diodes (by a factor of approximately 100 on a milliwatt basis), and the LLLT community is engaged in a vigorous ongoing debate about their respective benefits.
This review covers the mechanisms that are thought to operate at molecular and cellular levels in LLLT. Many of the most compelling applications of LLLT are in the field of neurology (both central and peripheral). Many serious brain diseases and injuries can be successfully treated with noninvasive transcranial laser therapy. Furthermore, in the peripheral nervous system, LLLT can be used effectively for nerve regeneration and pain relief.
CELLULAR AND MOLECULAR MECHANISMS OF LLLT
LLLT uses low-powered laser light in the range of 1-1000 mW, at wavelengths from 632-1064 nm, to stimulate a biological response. These lasers emit no heat, sound, or vibration. Instead of generating a thermal effect, LLLT acts by inducing a photochemical reaction in the cell, a process referred to as biostimulation or photobiomodulation. Photo-biology works on the principle that, when light hits certain molecules called chromophores, the photon energy causes electrons to be excited and jump from low-energy orbits to higher-energy orbits. In nature, this stored energy can be used by the system to perform various cellular tasks, such as photosynthesis and photomorphogenesis. Numerous examples of chromophores exist in nature, such as chlorophyll in plants, bacteriochlorophyll in blue-green algae, flavoproteins, and hemoglobin found in red blood cells. The respective colors of chromophores are determined by the part of the spectrum of light they absorb: chlorophyll is green, flavoprotein is yellow, and hemoglobin is red [5].
Mitochondria are considered the power generators of the eukaryotic cell, converting oxygen and nutrients through the oxidative phosphorylation process and electron transport chain into adenosine triphosphate (ATP), as shown in Figure 2. The basic idea behind cellular respiration is that high-energy electrons are passed from electron carriers, such as reduced nicotinamide adenine dinucleotide (NADH) and the reduced form of flavin adenine dinucleotide (FADH2), through a series of transmembrane complexes (including cytochrome c oxidase [CCO]) to the final electron acceptor, generating a proton gradient. The gradient is used by FOF1 ATP synthase to produce ATP. Various in vitro experiments, such as those that use rat liver isolates, found that cellular respiration was upregulated when mitochondria were exposed to an HeNe laser or other forms of illumination. Laser irradiation caused an increase in mitochondrial products (such as ATP [6], NADH, protein, ribonucleic acid [RNA] [7]) and a reciprocal augmentation in oxygen consumption. A similar effect is produced when tissue that contains mitochondria is exposed to low-level radiation. Visible and near-infrared (NIR) light is absorbed by the organelle, and an upregulation of cellular respiration is observed [8].
Illustration of mitochondrion, as well as of the electron transport chain and oxidative metabolism.
Once it was observed that LLLT's mechanism of action is at the level of the mitochondria, it remained to be determined what specific structure within the mitochondria acted as the chromophore. Four membrane-bound complexes have been identified in mitochondria, each constituting an extremely complex transmembrane structure embedded in the inner membrane. Complex IV, also known as CCO, is a large transmembrane protein complex found in mitochondria, which is a component of the respiratory electron transport chain (Figure 3). CCO appears to absorb the same spectrum of light as that observed for the action spectra for the biological response to light in the NIR range. Thus it is reasonable to assume that CCO acts as an important chromophore in LLLT [9]. CCO consists of 2 copper centers and 2 heme-iron centers that are capable of absorbing light over a wide range, including NIR.
Complex IV (cytochrome c oxidase) is the principal chromophore involved in low-level light therapy. It has 2 copper centers and 2 heme prosthetic groups. Cytochrome c is oxidized and oxygen is reduced to water during respiration.
The next reasonable question to consider is: What action does CCO modulate once it absorbs the energy from light? On the cellular level, LLLT may cause photodissociation of nitric oxide (NO) from CCO. In a stressed cell, NO produced by mitochondrial NO synthase displaces oxygen from CCO, which results in a downregulation of cellular respiration and a subsequent decrease in the production of energy-storing compounds, such as ATP. By dissociating NO from CCO, LLLT prevents the displacement of oxygen from CCO and thereby promotes unhindered cellular respiration [10] (see Figure 4). Increased CCO enzyme activity can be measured [11]; increased ATP production [12] and increased electron transport [13] also have been reported. The basic idea behind cellular respiration is that high-energy electrons are passed from electron carriers, such as NADH and FADH2, through a series of transmembrane complexes (including CCO) to the final electron acceptor. Increased cellular ATP produced by LLLT may contribute to the positive effects, both by raising cellular energy levels and by upregulating the cyclic AMP molecule (biochemically formed from ATP) that is involved in many signaling pathways.
Nitric oxide can bind to copper (or heme) centers in cytochrome c oxidase and inhibit respiration. The nitric oxide may be photodissociated by absorption of red or near infrared light, allowing oxygen to return and sharply increasing respiration and adenosine...
Oxygen acts as the final electron acceptor and is, in the process, converted to water. Part of the oxygen that is metabolized produces reactive oxygen species (ROS) as a natural by-product. ROS (eg, superoxide and hydrogen peroxide) are chemically active molecules that play an important role in cell signaling, regulation of cell cycle progression, enzyme activation, and nucleic acid and protein synthesis [14]. Because LLLT promotes the metabolism of oxygen, it also acts to increase ROS production. In turn, ROS activates certain redox-sensitive transcription factors such as nuclear factor-κB [NF-κB] and activator protein 1, which leads to the upregulation of various stimulatory and protective genes. The ultimate effect of LLLT is likely to be produced by transcription factor activation, which modulates the host's downstream cellular and tissue responses (see Figure 5).
Diagram that illustrates the mechanism of low-level light therapy (LLLT) on the cellular and molecular level. Near infrared light, absorbed by the mitochondria, causes upregulation of the cellular respiratory chain. A host of downstream cellular responses...
Almost certainly, other mechanisms through which LLLT produces its effects are at play in addition to the one just described. For example, NO is a potent vasodilator via its effect on cyclic guanine monophosphate production. Cyclic guanine monophosphate is also involved in many other signaling pathways. LLLT may cause the photodissociation of NO from intracellular stores (ie, nitrosylated forms of both hemoglobin and myoglobin, in addition to CCO) [15]. LLLT promotes the synthesis of deoxyribonucleic acid (DNA) and RNA [16] and increases the production of proteins [17]. It also modulates enzymatic activity [18], affects intracellular and extracellular pH [17,18], and accelerates cell metabolism [18,19]. The expression of multiple genes related to cellular proliferation, migration, and the production of cytokines and growth factors also have been shown to be stimulated by low-level light [20].
Light is a powerful force and has a myriad of effects. The specific mechanisms of action may vary among various clinical applications of LLL and will be discussed in the respective sections below. Furthermore, in spite of a great number of studies that explored how LLLT works, the exact mechanism of action remains to be fully elucidated.
STROKE
Transcranial LLLT (808 nm) has significantly improved recovery after ischemic stroke in rats when they received one treatment 24 hours after sustaining a stroke [21,22]. Stroke was induced in rats by 2 different methods: (1) permanent occlusion of the middle cerebral artery through a craniotomy or (2) insertion of a filament. The laser was used transcranially on the exposed (shaved skin) skull by placing the tip of the 4-mm diameter fiber optic onto the skin at 2 locations on the head (3 mm dorsal to the eye and 2 mm anterior to the ear) on the contralateral hemisphere to the stroke. These locations had been determined from prior measurements to be sufficient to illuminate 1 brain hemisphere as a result of dispersion of the laser beam by the skin and the skull. Results of previous studies had shown that LLLT of the contralateral, or both hemispheres, demonstrated no difference in functional outcome [23]. An NIR gallium arsenic diode laser was used transcranially to illuminate the hemisphere contralateral to the stroke at a power density of 7.5 mW/cm2 to the brain tissue [22]. In both models of stroke, the neurologic deficits at 3 weeks after stroke were significantly reduced (by 32%) (P < .01) in the laser-treated rats compared with control subjects.
In this study, the number of newly formed neuronal cells, assessed by double immunoreactivity to bromodeoxyuridine and tubulin isotype III, as well as migrating cells (double Cortin immunoreactivity), was significantly elevated in the subventricular zone of the hemisphere ipsilateral to the induction of stroke when treated by LLLT [21,22]. No significant difference in the stroke lesion area was found between control and laser-irradiated rats. The researchers suggested that an underlying mechanism for the functional benefit after LLLT in this study was possible induction of neurogenesis. Results of other studies also suggested that, because improvement in neurologic outcome may not be evident for 2-4 weeks in the poststroke rat model, delayed benefits may in part be due to induction of neurogenesis and migration of neurons [24,25]. In addition, transcranial LLLT may prevent apoptosis and improve outcomes by exerting a neuroprotective effect, although these exact mechanisms are poorly understood [26].
Other studies in rat and rabbit models also have observed that transcranial LLLT improves functional outcome after stroke [25,27,28]. A recent rabbit study combined transcranial LLLT with thrombolytic therapy by using tissue plasminogen activator, with no increase in bleeding and good safety [29].
In the aforementioned studies, it has long been hypothesized that increased mitochondrial function (ie, increased ATP production) in brain cells irradiated with NIR LLLT was one of the major mechanisms involved with the beneficial behavioral effects observed after LLLT treatment. A recent animal study with rabbits has shown a direct relationship between the level of cortical fluence (energy density) delivered (in J/cm2) and cortical ATP content in embolized rabbits [30]. Five minutes after embolization (right carotid), the rabbits were exposed to 2 minutes of NIR transcranial LLLT with use of an 808-nm laser source (continuous wave [CW] or pulsed wave [PW] at 100 Hz or at 1000 Hz on the skin surface, posterior to bregma at midline). Three hours after embolization, the cerebral cortex was excised and processed for measurement of ATP content. Embolization decreased cortical ATP content in ischemic cortex by 45% compared with naive rabbits.A linear relationship up to 4.5 J/cm2 in fluence delivered, was observed for the relationship between cortical fluence (in J/cm2) verus percent increase in cortical ATP content (over sham-treated embolized rabbits). This linear relationship was observed with a power density of 7.5 mW/cm2 CW (0.9 J/cm2), where an increase of 41% in cortical ATP was observed; and with a power density of 37.5 mW/cm2 PW (100 Hz, 4.5 J/cm2), where an increase of 157% in cortical ATP was observed. An increase in cortical ATP of 221% was observed with fluence of 31.5 J/cm2, delivered with a power density of 262.5 mW/cm2 PW, 1000 Hz. This suggests that a near-plateau effect was present regarding the fluence level delivered above 4.5 J/cm2. It was surprising, however, that the increased cortical ATP levels of 157% and 221%, were higher than those measured in naive rabbits that had never suffered stroke. Because the authors observed that the PW modes (100 Hz and 1000 Hz) were more effective than the CW mode to increase cortical ATP, they hypothesized that in future stroke studies in animals and in humans, even greater improvement in clinical rating scores might be achieved by optimizing the method of NIR transcranial LLLT delivery, including the length of treatment and the mode of treatment (PW).
Transcranial LLLT has been shown to significantly improve outcome in acute human stroke patients when applied approximately 18 hours after the stroke occurs over the entire surface of the head (20 points in the 10/20 electroencephalographic system), regardless of the stroke location [31]. Only one LLLT treatment was administered, and, 5 days later, significantly greater improvement was found in the real-treated group but not in the sham-treated group (P < .05, National Institutes of Health Stroke Severity Scale). This significantly greater improvement was still present 90 days after –the stroke occurred, at which time 70% of the patients treated with real LLLT had a successful outcome compared with only 51% of control subjects. An NIR (808 nm) laser was used, which delivered a fluence of 0.9 J/cm2 over the entire surface (2 minutes per each of the 20 points; power density of 7.5 mW/cm2).
In a second, similar study with the same transcranial LLLT protocol, an additional 658 acute stroke patients were randomly assigned to receive real or sham treatments of transcranial LLLT. Similar significant beneficial results (P < .04) were observed for the patients who had a moderate or moderate to severe stroke (n = 434) and received the real laser protocol but not for the patients who had a severe stroke [32]. When all 656 cases were included in the data analysis (including the severe stroke cases), no significant real versus sham LLLT effect was seen. When data for both stroke studies were pooled (n = 778 [120 plus 658]) [31,32], a highly significant beneficial effect was seen for the real transcranial LLLT group (P = .003) compared with those who received the sham laser treatment [33].
Lampl et al [31] wrote that “Although the mechanism of action of infrared laser therapy for stroke is not completely understood . . . infrared laser therapy is a physical process that can produce biochemical changes at the tissue level. The putative mechanism . . . involves stimulation of ATP formation by mitochondria and may also involve prevention of apoptosis in the ischemic penumbra and enhancement of neurorecovery mechanisms.”
To date, no studies have been conducted to examine transcranial LLLT treatment of chronic stroke patients. Naeser et al [34] studied the application of LLLT-laser acupuncture (instead of needles) to stimulate acupuncture points on the body in chronic stroke patients with paralysis. Seven stroke patients (range, 48-71 years; 5 men) were treated, 5 of whom had single left hemisphere stroke, and 2 of whom had single right hemisphere stroke. Five patients were treated for hemiplegia, including severely reduced or no voluntary isolated finger movement, and 2 patients had hand paresis only. Six of the 7 patients received laser acupuncture during the chronic phase after the stroke had occurred (10 months to 6.5 years after stroke onset), clearly beyond the spontaneous recovery phase, which is considered to be up to 6 months after the stroke occurs [35,36]. The patients served as their own controls; no sham LLLT was administered. One patient (who had hand paresis) received LLLT during the acute phase after the stroke occurred (1 month after the stroke occurred). The patients did not receive any physical therapy or occupational therapy treatments while participating in this study.
A 20-mW gallium aluminum arsenide (780 nm) NIR CW laser with a 1-mm-diameter aperture was used (Unilaser, Copenhagen, Denmark). (At the time of this study, more powerful red or NIR lasers were not yet available.) Treatment consisted of stimulation of shallow acupuncture points (located on the hands and face) for 20 seconds per point (51 J/cm2). Deeper acupuncture points (located on the arms and legs) were treated for 40 seconds per point (103 J/cm2). Acupuncture points were treated on both the paralyzed side (arm, leg, and/or face) and on the nonparalyzed side by using primarily acupuncture meridians of the large intestine, triple warmer, gall bladder, liver, small intestine, and stomach [34]. The patients were treated 2-3 times per week for 3-4 months. They received a total of 20, 40, or 60 treatments (based on patient availability and transportation). Within a few days before the first treatment and a few days after the last treatment, physical therapy and/or occupational therapy testing was performed by therapists blinded to the acupuncture treatment program to which the patient had been assigned: LLLT, real or sham needle, or no acupuncture. Overall, 5 of 7 of the patients (71.4%) showed improvement.
The 2 patients who showed no improvement had severe paralysis. We have observed that severity of paralysis and potential for improvement after LLLT-laser acupuncture (or needle acupuncture) is related to lesion location on chronic computed tomography (CT) scan acquired at least 3 months poststroke onset. Patients with lesion in more than half of the “periventricular white matter area” (PVWM) (adjacent to the body of the lateral ventricle, superior to the posterior limb, internal capsule), an area containing multiple efferent and afferent pathways (eg, thalamocortical, occipitofrontal, pathways from SMA/cingulate gyrus to the body of caudate, medial subcallosal fasciculus, and others), had severe paralysis which did not improve following LLLT-laser acupuncture (or needle) acupuncture treatments [34,37,38]. This area is diagrammed in Figure 6. The CT scan for a chronic stroke patient who had good response after LLLT-laser acupuncture treatments [34,37,38]. This area is diagrammed in Figure 7.
Location of periventricular white matter (PVWM) area (black arrow), adjacent to the body of the lateral ventricle, located immediately superior to the posterior limb, internal capsule (computed tomography slice angulation, coronal and axial views). An...
(a.) Computed tomography (CT) scan of a 65-year-old woman obtained 5 months after stroke onset shows sparing of the most posterior portion of the periventricular white matter (PVWM) (white arrow), that is, likely sparing of some of the leg fibers. This...
The 3 chronic stroke patients with hemiplegia who showed improvement after LLLT had an increase of 11%-28% in isolated, active range of motion for shoulder abduction, knee flexion, and/or knee extension (mean, 15.8%; SD, 7.1). This percentage increase after LLLT-laser acupuncture was similar to that observed after a series of 20 or 40 needle acupuncture treatments [37,38]. The person with hand paresis who was treated with LLLT at 33 months after stroke onset showed an increase of 2-6 lb in grip strength, 3-jaw chuck, tip pinch, and lateral pinch in the affected hand. These results are similar to those obtained with needle acupuncture [39]. These findings are intriguing and suggest that some recovery of motor function can occur with needle acupuncture or LLLT acupuncture applied to body acupuncture points in chronic stroke patients.
A reduction in hand spasticity also has been observed when chronic stroke patients are treated with a combination of red-beam laser applied to hand acupuncture points plus microamps transcutaneous electrical nerve stimulation (TENS). Figure 8 shows an immediate reduction in hand spasticity after the first hand treatment when LLLT-laser acupuncture and microamps TENS were used with 2 chronic stroke patients. This LLLT and microamps TENS hand treatment program also may be used with patients who have hand spasticity related to other etiologies, including, for example, traumatic brain injury (TBI), “stiff man syndrome,” and spinal cord injury (SCI) (personal observation, M.A.N., 2001). Similar to red and NIR LLLT, microamps TENS increases ATP levels when applied to the skin [40]. However, Cheng et al [40] observed that when stronger milliamps TENS was used (eg, similar to conventional TENS), the ATP levels were decreased. Hence when microamps TENS is used (as shown in Figure 8) [41], it is advisable to keep the sensation below threshold for the patient to increase ATP (not decrease ATP).
(a.) Before the first low-level laser therapy (LLLT) and microamps transcutaneous electrical nerve stimulation (TENS) acupuncture treatment. It was 1.5 years after stroke onset and the patient still had right hand spasticity and was unable to extend her...
TRAUMATIC BRAIN INJURY
Each year in the United States, more than 1.4 million new cases of TBI occur, and more than 80,000 persons are left with permanent disability [42]. Mild TBI (mTBI) from single and multiple events is the most frequent type of head injury experienced by military personnel deployed to Iraq and Afghanistan [43]. TBI is known to cause damage that ranges from observable to microscopic throughout the gray and white matter of the brain. Diffuse axonal injury [44] is often observed in the anterior corona radiata and frontotemporal regions [45]. Two regions highly susceptible to damage within the frontal lobes are the prefrontal cortex and the anterior cingulate gyrus. Cognitive processing problems result from tissue damage and inefficient cellular function in these brain regions. The prefrontal cortex is involved with maintaining, monitoring, and manipulating information in working memory [46] and particularly in sustained attention [47,48].
In the first reported study of the use of transcranial LLLT to treat traumatic brain injury, an animal model was used [49]. Mice were subjected to closed-head injury (CHI) by using a weight-drop procedure, and 4 hours after CHI, either sham or real NIR LLLT (808 nm) was administered transcranially. The control group received no laser therapy (n = 8); the laser-treated group (n = 16) received 1 transcranial LLLT treatment by using a 200-mW, 808-nm NIR laser with a 3-mm-diameter probe tip (Photothera Inc, Carlsbad, CA). Either 10 or 20 mW/cm2 was administered. A single point was treated on the skull (a skin incision was made) that was located 4 mm caudal to the coronal suture line on the midline. The point was treated for 2 minutes (1.2-2.4 J/cm2). At 24 and 48 hours after CHI, no significant difference in motor behavior was seen between mice in the laser-treated and control groups. After 5 days, the motor behavior was significantly better (P < .05) in the laser-treated group; in addition, the neurobehavioral scores were 26%-27% better (lower scores indicated better motor behavior). At 28 days after CHI, the brain-tissue volume was examined for mice in each group. The mean lesion size of 1.4% in the laser-treated group (SD 0.1) was significantly smaller (P < .001) than in the control group (12.1%, SD 1.3). No difference in lesion size or behavior was observed in the mice treated with 10 mW/cm2 and those treated with 20 mW/cm2. The researchers suggested various possible mechanisms, including an increase in ATP, total antioxidants, angiogenesis, neurogenesis, heat shock proteins content, and an antiapoptotic effect, similar to observations reported after LLLT treatment of ischemic heart skeletal muscles [50-54].
Moreira et al [55] conducted a study in 2009 using phototherapy with low-intensity lasers and observed the effect on local and systemic immunomodulation after cryogenic brain injury in rats. Brain and blood samples were analyzed by enzyme-linked immunosorbent assay for the production of cytokines interleukin (IL)-6 , IL-10, IL-1b, and tumor necrosis factor (TNF)-α. The study concluded that laser phototherapy could positively affect the balance of IL-1b, TNF-α, and IL-6 in rats and thereby prevent cell death after TBI.
Wu et al [56] reported another mouse study of LLLT mediated by transcranial laser therapy. A nonfocal (diffuse) TBI was produced by a CHI caused by a calibrated weight-drop device. A neurologic severity score for each mouse was determined based on 10 standardized performance tests (involving beam balancing and maze exiting) administered at specified times. Mice with a neurologic severity score of 7-8 (moderately severe brain injury) were used in the study. Mice were given a single treatment to the top of the head with 36 J/cm2 of a 665-nm, 810-nm, or 980-nm laser 4 hours after the closed head TBI. Both 665-nm and 810-nm lasers were highly effective in improving the neurologic performance of the mice during the succeeding 4 weeks. The 980-nm wavelength was ineffective (negative control). We believe that this difference in results can be explained by the absorption spectrum of the different chromophores; CCO has peaks at 660 nm and 810 nm, whereas water has a peak at 980 nm.
In humans, 2 persons with chronic mTBI recently have been reported to have improved cognition after a series of treatments with transcranial, red, and NIR LEDs [57,58]. The LED cluster heads were applied to the forehead and scalp areas (the hair was not shaved off but was parted underneath each 2-inch-diameter LED cluster head). Each cluster head had 61 diodes (9 red 633-nm diodes and 52 NIR 870-nm diodes). Each diode was 12-15 mW, and the total power output was 500 mW. The LED cluster heads were applied to bilateral frontal, parietal, and temporal areas and to the mid-sagittal suture line.
Each LED cluster head was applied for 10 minutes per placement. With the device used here (parameters described above), 1 joule per cm2 (J/cm2) energy density was produced during every 45 seconds of exposure time. The energy density dose at the forehead-scalp was 13.3 J/ cm2; the power density was 22.2 mW/cm2 (±20%). The power density refers to the mW of power applied per cm2. The ± refers to the range of fluctuation (plus or minus 20%) on the power density per cm2. This power density is well below that used in other transcranial laser or LED studies to treat acute stroke cases or severe depression cases (225 mW/cm2) [59]. It is estimated that only approximately 3% of the photons delivered to the forehead-scalp surface will reach 1 cm, to the cortex [60]. The dose of 13.3 J/cm2 per placement area was estimated to deliver only 0.4 J/cm2 to the brain cortex. No sensation of heat or pain was reported during the LED application to the skin or scalp. These LED cluster heads (MedX Health Corp, Mississauga, Ontario, Canada) are approved by the U.S. Food and Drug Administration for treatment of musculoskeletal pain; they were used off-label for treatment of cognition in the mTBI cases. No potential existed for ocular damage because the LEDs produce noncoherent light. These LED cluster heads also have been approved by the Food and Drug Administration for home treatment.
A 66-year-old woman (case 1) began transcranial LED treatments 7 years after a motor vehicle–related TBI. Before LED treatment, she could focus on her computer for only 20 minutes. After 8 weekly LED treatments, her focused computer time increased to 3 hours. She has treated herself nightly at home for 5.5 years, with transcranial LED. She maintains her improved cognition at age 72 years.
Case 2 involved a 52-year-old retired, high-ranking female military officer who had a history of multiple TBIs. Her brain MRI showed frontoparietal atrophy. She was medically disabled for 5 months before beginning nightly transcranial LED treatments at home (see Figure 9, A and B). After 4 months of nightly LED treatments, she returned to work full time as an executive consultant for an international technology consulting firm and discontinued medical disability. Neuropsychological tests performed after 9 months of transcranial LED showed significant improvement in cognition (see Figure 9, C). After LED treatments, she improved on tests of executive function (inhibition and inhibition accuracy, +2 SD) and on memory (immediate and delayed recall +1, +2 SD). The improvement of +1 or +2 standard deviations on her scores refers to the degree of improvement on her scores after 9 months of LED treatments (versus before LED treatments). The SDs are provided with the test materials, and they are based on the published norms for each test.
(a.) Red and near-infrared (NIR) light-emitting diode (LED) cluster head (2-inch diameter) for transcranial LED treatments. (b.) Sample placement location on right forehead for one of the LED cluster heads during transcranial LED treatment. (c.) Graph...
Both patients with TBI reported that they needed to continue with home treatments. If they stop treatment for 1 or 2 weeks, then their cognitive problems started to return. Both patients with TBI reported improved sleep. The second patient with TBI reported a decrease in her posttraumatic stress disorder symptoms after a few months of using the transcranial LEDs, and Schiffer et al [59] also reported a reduction in posttraumatic stress disorder symptoms in 3 of 10 patients with major depression who were treated with transcranial LED.
Several possible mechanisms may be associated with the improved cognition in the mTBI cases treated with transcranial LEDs [58]. Mitochondria display a significant amount of dysfunction after TBI [61-63]. The primary mechanism for improvement posited in one study with human acute stroke patients was an increase in ATP, with photons being used by CCO in the mitochondria to increase ATP, especially in the cortex [64].
An increase in ATP after red and/or NIR LED treatments in patients with chronic TBI would have beneficial effects, including an increase in cellular respiration and oxygenation. Oxidative stress plays a role in the damage present after TBI [65]. One hypothesis is that LLLT produces low levels of ROS in mitochondria of illuminated cells and that these ROS cause NF-κB activation via the redox sensitive sensor enzyme protein kinase D1, which results in upregulation of the mitochondrial superoxide dismutase [66]. A single exposure of LLLT-LED in vitro with fibroblasts has been observed to increase NF-κB in the short term [67]. In stimulated dendritic cells in the longer term, however, NF-κB and pro-inflammatory cytokines were reduced [68]. Thus, in the long term, repeated LED treatments are hypothesized to decrease inflammation (less NF-κB) and upregulate gene products that are cytoprotective, such as superoxide dismutase, glutathione peroxidase, and heat shock protein 70 [54,69]. It is hypothesized that an overall protective response occurs with repeated LED treatments and that major ROS-mediated damage and chronic inflammation that occur in the brain after TBI may actually be reduced.
Acupuncture points located on the scalp were treated with the red-NIR LEDs [57]. This includes points along the Governing Vessel (GV) acupuncture meridian, located on the midline of the skull (including, in part, the mid-sagittal suture line). Some acupuncture points located on the GV meridian have been used historically to help treat patients in coma [70] and stroke [71], for example, GV 16 (inferior to occipital protuberance), GV 20 (vertex), and GV 24 (near center-front hairline); these points were treated in both patients with TBI reported in this study.
Transcranial red-NIR LED may have irradiated the blood via the valveless, emissary veins located on the scalp surface but interconnecting with veins in the superior sagittal sinus (M. Dyson, oral personal communication, June 2009). If red-NIR photons penetrate deeply enough to reach the cortex, then it also is possible they are entering small vessels located between the arachnoid and the pia mater, including those that supply arterial blood to superficial areas of the cortex. Direct in vitro blood irradiation with a red-beam laser has been observed to improve erythrocyte deformability (flexibility) and rheology [72,73]. A beneficial effect from direct-laser blood irradiation in vivo has been observed during stenting procedures where a low-level, red-beam laser (10 mW, 650 nm) was used, with the beam placed directly into a coronary artery [74]. The restenosis rate was reduced and no adverse effects or complications were noted. Thus blood irradiation at the scalp may have affected local intracerebral blood and circulation; however; whether this effect occurred is unknown and would require further study.
An increase in regional cerebral blood flow may have occurred, specifically to the frontal lobes. The second TBI case showed significant improvement on objective, neuro-psychological testing for executive function (inhibition) after administration of LED. These results suggest improved function in the prefrontal cortex and anterior cingulate gyrus regions. Significant improvement on “inhibition” on the Stroop test particularly suggests improved function of the medial prefrontal cortex, anterior cingulate gyrus area [75]. It is possible that this medial prefrontal cortex area could have been treated with NIR photons, especially when the LED cluster head was placed over the midline, front hairline area. The dorsolateral prefrontal cortex also was likely irradiated when the LEDs were placed on the left and right high-frontal areas of the scalp. Increased regional cerebral blood flow also could have occurred in frontal pole areas with the TBI cases, as was observed in the recent transcranial LED study to treat major depression [59]. Additional controlled studies with real and sham transcranial LLLT and LED are recommended to investigate whether these methods can be applied to improve cognition and reduce symptom severity in persons with acute and chronic TBI. The LED technology is not expensive ($1400 for a single LED cluster head and approximately $4000 to $5000 for a unit with 3 LED cluster heads). The transcranial LED treatment protocol can be used in the home.
DEGENERATIVE CENTRAL NERVOUS SYSTEM DISEASE
The positive effects of transcranial laser therapy on stroke and TBI have led to early investigations into whether LLLT may have benefits for persons with degenerative brain disorders, which are a rapidly growing affliction of the world's aging population. Moges et al [76] tested whether LLLT had a role to play in treating familial amyotrophic lateral sclerosis (FALS), which is a neurodegenerative disease characterized by progressive loss of motor neurons and death. Mitochondrial dysfunction and oxidative stress play an important role in motor neuron loss in ALS. The study combined LLLT (with use of an 810-nm diode laser with 140-mW output power targeting a 1.4-cm2 spot area for 120 seconds using 12 J/cm2 energy density) and riboflavin to test the survival of motor neurons in a mouse model of FALS. Motor function (determined with use of the Rota rod test) was significantly improved in the LLLT group in the early stage of the disease. Immunohistochemical expression of the astrocyte marker glial fibrillary acidic protein was significantly reduced in the cervical and lumbar enlargements of the spinal cord as a result of LLLT.
Trimmer et al [77] carried out preliminary studies that may have relevance to Parkinson disease (PD). Mitochondria supply the ATP needed to support axonal transport, which contributes to many other cellular functions essential for the survival of neuronal cells. Furthermore, mitochondria in PD tissues are metabolically and functi
Photobiomodulation (PBM) also known as low-level laser (or light) therapy has been known for over 50 years (since
1967), but it is only relatively recently that it has begun to make the transition into the mainstream. PBM describes the
use of red or near-infrared light at levels that do not produce undue heating of the tissue to produce beneficial effects
on the human body. The introduction of light-emitting diodes (LEDs) has made this approach more accessible than the
previously used laser sources, as LEDs are safer, cheaper, and can easily be used at home. Another factor that has led
to PBM becoming more widely accepted is the growing understanding of the mechanisms of action at a molecular and
cellular level. The lack of a clear mechanism of action was a deterrent to many biomedical scientists who maintained a
healthy level of skepticism.
Among the wide range of tissues, organs, diseases, and conditions that can be beneficially affected by PBM, the subject
of this book is the brain. The brain is probably the single human organ that engenders the most concern, interest,
and expenditure in the 21st century. Brain disorders that cause widespread morbidity, mortality, and loss of quality of
life can be divided into four broad categories. Traumatic brain disorders include stroke, traumatic brain injury (TBI),
global ischemia, and perinatal difficulties. Neurodegenerative diseases include Alzheimer’s disease, Parkinson’s disease,
and a range of dementias. Psychiatric disorders include major depression, anxiety, addiction, and insomnia, among
many others. Finally there are neurodevelopmental disorders (autism and ADHD) and the possibility of cognitive
enhancement in healthy individuals. Many of these brain disorders are specifically addressed in the present volume.
The book is divided into three parts. The first part covers some basic considerations, dosimetry, and devices, and
discusses the mechanisms of action at a cellular level and on the brain as a whole organ. The second part includes contributions
from researchers who have carried out studies on a variety of animal models in their investigations of brain
disorders, stroke, TBI, and Alzheimer’s and Parkinson’s diseases, to name a few. The third part concentrates on human
studies, including controlled clinical trials, pilot trials, case series, and clinical experience. Disorders treated include
TBI, stroke, Alzheimer’s and Parkinson’s diseases, depression, and others.
The book is expected to play a role in stimulating the further increase and acceptance of PBM for brain disorders,
which has really started to take off in recent years. It will also act as a resource for researchers and physicians wishing
to get a broad overview of the field and who are contemplating entering it themselves. The number of individuals considering
obtaining a home-use PBM device is also steadily increasing and this book will act as Original Source: https://books.google.com/books/about/Photobiomodulation_in_the_Brain.html?id=P0qiDwAAQBAJ&source=kp_book_description
Near-infrared light increases ATP, extends lifespan and improves mobility in aged Drosophila melanogaster
Rana Begum 1 , Karin Calaza 2 , Jaimie Hoh Kam 1 , Thomas E. Salt 1 , Chris Hogg 3 and Glen Jeffery - Royal Society Publishing (Publication) 4509 PBM increased the average lifespan and mobility of fruit flies. Although they all died at 12 weeks, treating the flies with PBM significantly increase the average healthspan.
Near-infrared light increases ATP, extends lifespan and improves mobility in aged Drosophila melanogaster Rana Begum 1 , Karin Calaza 2 , Jaimie Hoh Kam 1 , Thomas E. Salt 1 , Chris Hogg 3 and Glen Jeffery Institute of Ophthalmology, University College London, London EC1V 9EL, UK 2 Program of Neuroscience, Institute de Biologia, Universidade Federal Fluminense, Rio de Janeiro 24210130, Brazil 3 Moorfields Eye Hospital, London EC1V 2PD, UK Ageing is an irreversible cellular decline partly driven by failing mitochondrial integrity. Mitochondria accumulate DNA mutations and reduce ATP production necessary for cellular metabolism. This is associated with inflammation. Near-infrared exposure increases retinal ATP in old mice via cytochrome c oxidase absorption and reduces inflammation. Here, we expose fruitflies daily to 670 nm radiation, revealing elevated ATP and reduced inflam- mation with age. Critically, there was a significant increase in average lifespan: 100–175% more flies survived into old age following 670 nm exposure and these had significantly improved mobility. This may be a simple route to extending lifespan and improving function in old age. 1. Introduction Mitochondria provide cellular energy via adenosine triphosphate (ATP). But, their DNA (mtDNA) suffers from progressive mutations resulting in reduced ATP production, which is thought to run concomitantly with an increase in pro-inflammatory reactive oxygen species (ROS) [1,2]. Hence, hallmarks of ageing are reduced cellular energy and progressive systemic inflammation. Meta- bolic demand also plays a role as tissues and organisms with high metabolic rates generally suffer from rapid ageing [3,4]. The retina has the greatest metabolic demand in the body [5], but ATP decline in the central nervous system can be significantly improved by near-infrared/infrared light (NIR/IR, [6]). Specific wavelengths in this range are absorbed by cytochrome c oxidase in mitochondrial respiration, improving its efficiency [7–10]. These wavelengths improve mito- chondrial membrane potentials, significantly reduce inflammation and reduce macrophage numbers with brief exposures of around 60–90 s repeated over approximately a week [11,12]. NIR/IR also reduces experimental pathology when insult impacts on mitochondrial function, as in experimental Parkinson’s disease, where NIR significantly reduces cell death in the substantia nigra [13]. However, NIR/IR studies have largely used light for short periods and their impact on lifespan has not been assessed [7,11,12]. If NIR improves mitochondrial function we predict it may extend life. The fly has been used here because of its relatively short life [14]. Hence, we ask if long-term exposure to 670 nm in Drosophila melanogaster can increase lifespan and improve function in old age. 2. Material and methods Drosophila melanogaster were used. Hatched male flies were housed on 12/12 light cycle at 258C within a season. Half were exposed to 670 nm for 20 min per day at & 2015 The Authors. Published by the Royal Society under the terms of the Creative Commons Attribution License http://creativecommons.org/licenses/by/4.0/, which permits unrestricted use, provided the original author and source are credited. on March 18, 2015http://rsbl.royalsocietypublishing.org/Downloaded from 40 mW cm 22 in clear plastic 50 cm 3 (28 mm wide) containers, illuminating flies from either side, which were counted weekly. Room illumination was 2 mW cm 22 . 670 nm energies were approximately 100 times lower than indirect sunlight, consistent with earlier studies [7]. Light devices were built by C. H. Elec- tronics UK and contained 50 670 nm LEDS over 20 cm 2 . Six independent replicates were used in lifespan experiments (n ¼ 620 flies). ATP, inflammation and mobility were assessed at seven weeks, when ATP and mobility are known to decline [15]. ATP was measured by luciferin–luciferase assay (Enliten w ATP Assay System, Promega). Flies were killed with liquid nitrogen, transferred to 2.5% trichoroacetic acid (TCA), then homogenized at 48C. Supernatant was collected and the TCA was neutralized with 1 M Tris–acetate buffer (pH 7.75, final TCA concentration 0.0625%); 10 ml of neutralized solution was added to 100 ml of luci- ferin–luciferase in fresh buffer. ATP was measured using an Orion microplate luminometer (Berthold Detection Systems GmbH) and data normalized to fly numbers. Tissues were homogenized in 2% sodium dodecyl sulfate (SDS) with protease inhibitor cocktail for Western blot (Roche Diagnos- tics), and centrifuged; the supernatant was pipetted out, separated with 10% SDS–PAGE and electrophoretically transferred onto nylon membranes. Immunoblotting was undertaken for complement component C3 (Cappel, MP Biomedicals), which is highly conserved [16]. Protein was quantified by densitometric X-ray scanning and values were normalized to a-tubulin. Fly mobility assessment was as Bjedov et al. [14]. Flies were placed in 100 ml clear cylinders (seven flies per trial), tapped to the bottom and then videoed, the last two steps repeated three times. Using the videos, the number of flies above the 50 ml mark (9 cm from the bottom) was counted after 1 min. Individual flies were traced, with absolute distance travelled measured. Data w er e analysed with GraphPad P RISM v. 5 and sta t is ti cal analysis was undertaken using Mann –Whitne y U non-parametric and log-rank tests. 3. Results (a) ATP levels are elevated and systemic inflammation reduced Whole body ATP declines with age only after appr o xima tely seven weeks [14], when ATP was measured here. A TP concen- trations wer e significantly grea t er, by approxima tely 80%, in 670 nm exposed animals compared with unexposed (figure 1a, Mann–Whitney test p ¼ 0.028). At seven weeks, W estern blots wer e undertaken for inflammatory marker complement com- ponent C3. This was reduced in 670 nm exposed flies compared with controls (figure 1b). Hence, 670 nm radiation elevates ATP and reduces inflammation. (b) Lifespan increases Fly numbers in experimental and control groups were similar in the two weeks post-hatching. From week 3, fly deaths were greater in controls than 670 nm exposed flies and they remained so at each time point until week 11–12, when all flies were dead in both groups. This difference was significant (figure 2, log-rank test p ¼ 0.008). The progressive mean percentage increase in 670 nm flies alive over controls is given in figure 2b. Group differences accelerated from week 4, when 10% extra 670 nm treated flies were alive compared with controls, to approximately 50% extra when the control population had halved. By the time the control population was reduced by 80%, at week 8, more than 100% extra 670 nm treated flies remained alive. Subsequently, group differences reached almost 180% before declining to zero in both groups at week 11–12. Hence, 670 nm did not extend absolute lifespan. (c) Aged mobility increases Mobility of 670 nm treated and control flies was measured at seven weeks. Significantly more 670 nm treated flies climbed above the 50 ml level (9 cm) and significantly more travelled a greater distance than controls (Mann–Whitney test p ¼ 0.028, p ¼ 0.014, respectively). Twice as many 670 nm flies climbed above 50 ml (9 cm) compared with controls and these travelled twice the distance in 1 min compared with controls (figure 2c,d). Hence, 670 nm exposure significantly improves both lifespan and mobility. 4. Discussion Drosophila melanogaster has been widely used in lifespan studies as they are short lived and their genomic sequence is relatively well understood [14,17], hence their adoption experimentally here to extend lifespan. Our results reveal [ATP] (nM)/fly ATP level(a) C3 expression (Western blot)(b) control absolute intensity 670 control 670 control C3 ~ 110 kDa a-tubulin 55 kDa 670 * 0 0 500 1000 200 400 600 Figure 1. Exposur e to 670 nm radiation increases ATP in aged flies and reduces inflammati on. (a) Sev en week old flies exposed to 670 nm had a significant incr ease in whole body ATP compared with controls, p ¼ 0.028. n ¼ 25 flies per group. (b) Whole body inflammation (C3) was measured in seven week flies using W estern blot. This was reduced in 670 nm exposed flies by approxima tely 15%. Here, flies were pooled within groups as C3 protein levels were lo w in individuals. Hence there are no error bars. n ¼ 15 flies per group. (Online version in colour.) rsbl.royalsocietypublishing.org Biol. Lett. 11: 20150073 2 on March 18, 2015http://rsbl.royalsocietypublishing.org/Downloaded from that when flies are exposed to 670 nm radiation they have reduced inflammation, improved ATP, improved mobility and extended average lifespans. These data are consistent with the majority of studies undertaken using 670 nm on mammals, showing reduced inflammation in experimental models and in ageing, and improved ATP levels [6,7]. How- ever, it would be difficult to undertake lifespan experiments in mice as the light would not penetrate the entire body as it does in flies and hence its influence would not be systemic. There are many factors and pathways in ageing, and nine candidate hallmarks have been suggested, which may be separate, but also are likely to have interactions [1]. Mito- chondrial function is one. Previously, mitochondrial function and ageing were viewed within a framework of pro- gressive mtDNA mutations/deletions resulting in reduced ATP and increased ROS. The balance of these factors was seen as a driver in the mitochondrial theory of ageing [18]. However, evidence has undermined the role of ROS in ageing [19,20]. Hence, some mutant mice have reduced life- span as a result of mtDNA mutations/deletions not associated with increased ROS [21,22]. Further, increased ROS can prolong lifespan in yeast and Caenorhabditis elegans [22,23], and in mammals it does not accelerate ageing [20]. These data are reviewed by Lopez-Otin et al. [1], who argue that low ROS may activate compensatory mechanisms and not directly contribute to ageing. Such data may undermine the ROS element in Harman’s mitochondrial theory [18]. If correct, it places greater potential emphasis on ATP in ageing. NIR has been successful in treating induced pathology [7] and ageing, particularly in the retina, where progressive age- related inflammation is marked owing to high metabolic rate [11,12]. These wavelengths penetrate deeply and 670 nm trans-illuminated our flies at 40 mW cm 22 . In relation to this, it may be significant that, while old domestic incandescent light- ing contained significant NIR elements, none is present in modern strip lighting or energy-saving domestic lighting [12]. The absence of these wavelengths from artificial lighting may have long-term consequences. As longer wavelengths penetrate deeply, this may be of significance not only for the ageing eye, but also potentially for other tissues. Ethics statement. Fly research is free of legal ethical constraint. Data accessibility. All data are presented in the manuscript. Acknowledgement. We thank Iris Salecker, Giovanna Vinti and Tobi Weinrrich for technical assistance. Author contributions. G.J. designed experiments and wrote the manu- script. All authors undertook the experiments and approved the final version of the manuscript. R.B. analysed the data. Funding statement. Supported by the Rosetrees Trust UK. K.C. was a research fellow from CAPES Brazil (proc. 18134/12-2). Competing interests. We have no competing interests. References 1. Lopez-Otin C, Blasco MA, Partridge L, Serrano M, Kroemer G. 2013 The hallmarks of aging. Cell 153, 1194–1217. (doi:10.1016/ j.cell.2013.05.039) 2. Balaban RS, Nemoto S, Finkel T. 2005 Mitochondrial, oxidants and aging. Cell 120, 483–495. (doi:10.1016/j.cell.2005.02.001) 3. Speakman JR. 2005 Body size, energy, metabolism and lifespan. J. Exp. Biol. 208, 1717–1730. (doi:10. 1242/jeb.01556) 4. Wang Z, Ying Z, Bosy-Westphal A, Zhang J, Schautz B, Later W, Heymsfield SB, Mu¨ller MJ. 2010 Specific metabolic rates of major organs and tissues across adulthood: evolution by mechanistic model of resting expenditure. Am. J. Clin. Nutr. 92, 1369– 1377. (doi:10.3945/ajcn.2010.29885) 5. Yu DY, Cringle SJ. 2001 Oxygen distribution and consumption within the retina in vascularized and avascular retinas and in animal models of disease. Prog. Retin. Eye Res. 20, 175–208. (doi:10.1016/ S1350-9462(00)00027-6) 0 0 10 20 30 40 50 60 70 80 100 (a) (c) (d ) (b) % survival over controls n = 620 flies fly survival curves for 670 nm (–) and control (–) 90 123456 time (weeks) % survival 78910 0 0 100 200 300 123456 no. weeks % increase over control control distance travelled in 1 min 670 control 670 * 0 20 60 40 80 100 distance (mm) fly climbing (>90 mm) * 0 20 60 40 80 % >90 mm in 1 min 78910 11 12 Figure 2. Lifespan and mobility. (a) Fly numbers at progressive weeks in groups exposed to 670 nm supplemented light each day (red line) and controls (black line). Curves are averages for six independent experiments with a minimum of 40 flies per group in each experiment. Fly death rates separated between three and six weeks with fewer flies dying in 670 nm exposed animals. Reduction in the two population followed similar patterns from six weeks but with the 670 nm exposed group having greater numbers at any point until week 12. In all replicates, there was no indication that 670 nm increased absolute lifespan beyond weeks 11 – 12. Differences between the two groups were statistically significant ( p ¼ 0.008). (b) Inset: percentage increase of 670 nm exposed flies alive at pro- gressive weeks. (c) Seven week old 670 nm exposed flies were more active than controls. (d) Mobility measures the percentage of flies that climbed above 90 mm in a clear 100 ml cylinder. (d) This was filmed and then the distance travelled by each fly was measured in each group. In both cases, the 670 nm exposed flies where significantly more mobile. There were 21 flies in each group in each condition. (Online verion in colour.) rsbl.royalsocietypublishing.org Biol. Lett. 11: 20150073 3 on March 18, 2015http://rsbl.royalsocietypublishing.org/Downloaded from 6. Gkotsi D, Begum R, Salt T, Lascaratos G, Hogg C, Chau KY, Schapira AH, Jeffery G. 2014 Recharging mitochondrial batteries in old eyes. Near infra-red increases ATP. Exp. Eye Res. 122, 50 –53. (doi:10. 1016/j.exer.2014.02.023) 7. Fitzgerald M et al . 2013 Red/near-infrared irradiation therapy for treatment of central nervous system injuries and disorders. Rev. Neurosci. 24, 205–226. (doi:10.1515/revneuro-2012-0086) 8. Wilson M, Greenwood C. 1970 The long-wavelength absortion band of cytochrome c oxidase. Biochem. J. 116, 17 –18. 9. Karu TI, Pyatibrat LV, Kolyakov SF, Afanasyeva NI. 2005 Absorption measurements of cell monolayer relevant to phototherapy: reduction of cytochrome c oxidase under near IR radiation. J. Photochem. Photobiol. 81, 98– 106. (doi:10.1016/j.jphotobiol.2005.07.002) 10. Cooper CE, Springett R. 1997 Measurement of cytochrome oxidase and mitochondrial energetics by near-infrared spectroscopy. Phil. Trans. R. Soc. Lond. B 352, 669– 676. (doi:10.1098/rstb.1997.0048) 11. Kokkinopoulos I, Colman A, Hogg C, Heckenlively J, Jeffery G. 2013 Age-related inflammation is reduced by 670 nm light via increased mitochondrial membrane potential. Neurobiol. Aging 34, 602– 609. (doi:10.1016/j.neurobiolaging.2012.04.014) 12. Begum R, Powner MB, Hudson N, Hogg C, Jeffery G. 2013 Treatment with 670 nm up regulates cytochrome C oxidase expression and reduces inflammation in an age-related macular degeneration model. PLoS ONE 8, e57828. (doi:10. 1371/journal.pone.0057828) 13. Purushothuman S, Nandasena C, Johnstone DM, Stone J, Mitrofanis J. 2013 The impact of near- infrared light on dopaminergic cell survival in a transgenic mouse model of parkinsonism. Brain Res. 1535, 61 –70. (doi:10.1016/j.brainres.2013.08.047) 14. Bjedov I, Toivonen JM, Kerr F, Slack C, Foley A, Partridge L. 2010 Mechanisms of life span extension by rampamycin in the fruit fly Drosophila melanogaster. Cell Metab. 11, 35–46. (doi:10.1016/ j.cmet.2009.11.010) 15. Vernace VA, Arnaud L, Schmidt-Glenewinkel T, Figueiredo-Pereira ME. 2007 Aging perturbs 26S proteasome assembly in Drosophila melanogaster . FASEB J. 21, 2672–2682. (doi:10.1096/fj.06- 6751com) 16. Nonaka M, Kimura A. 2006 Genomic view of the evolution of the complement system. Immunogenetics 58, 701– 713. (doi:10.1007/ s00251-006-0142-1) 17. Celniker SE, Rubin GM. 2003 The Drosophila melanogaster genome. Annu. Rev. Genomics Hum. Genet. 4, 89–117. (doi:10.1146/annurev.genom.4. 070802.110323) 18. Harman D. 1981 The ageing process. Proc. Natl Acad. Sci. USA 78, 7124 –7128. (doi:10.1073/pnas. 78.11.7124) 19. Edgar D et al. 2009 Random point mutations with major effects on protein coding genes are the driving force behind premature aging in mtDNA mutator mice. Cell Metab. 10, 131–138. (doi:10. 1016/j.cmet.2009.06.010) 20. Hiona A et al. 2010 Mitcohondrial DNA mutations induce mitochondrial dysfunction, apoptosis and sarcopenia in skeletal muscle of mitochondrial mutator mice. PLoS ONE 5, e11468. (doi:10.1371/ journal.pone.0011468) 21. Doonan R, McElwee JJ, Matthijssens F, Walker GA, Houthoofd K, Back P, Matscheski A, Vanfleteren JR, Gems D. 2008 Against the oxidative damage theory of aging: superoxide disumatases protect against oxidative stress but have little or no effect on life span in Caenorhabditis elegans. Genes Dev. 22, 3236–3241. (doi:10.1101/gad. 504808) 22. Mesquita A et al. 2010 Caloric restriction or catalase inactivation extends yeast chronological lifespan by inducing H 2 O 2 and superoxide dismutase activity. Proc. Natl Acad. Sci. USA 107, 15 123–15 128. (doi:10.1073/pnas.1004432107) 23. Zhang Y et al. 2009 Mice deficient in both Mn superoxide dismutase and glutathione peroxidase-1 have increased oxidative damage and a greater incidence of pathology but no reduction in longevity. J. Gerontol. A Biol. Sci. Med. Sci. 64, 1212– 1220. (doi:10.1093/gerona/glp132) rsbl.royalsocietypublishing.org Biol. Lett. 11: 20150073 4 on March 18, 2015http://rsbl.royalsocietypublishing.org/Downloaded from
TheraLazr Cold Laser Treatment of Parkinson Tremor
Dr. Stephen Riner D.C. - YouTube 2012 (Video) 4321 Dr. Riner uses LLLT to treat a patient with Parkinsons, the video shows the progression of the treatment
This video shows before and after treatment footage of a patients with advanced Parkinsons. Treatment lasts about 2 weeks. Dr Riner is using the brain and neurostim setting on the brain, C5 Nerve Root and the Ulnar nerve in the elbow.
The TheraLazr is the prototype for the Avant LZ30 series of lasers.
“Quantum Leap” in Photobiomodulation Therapy Ushers in a New Generation of Light-Based Treatments for Cancer and Other Complex Diseases: Perspective and Mini-Review
Luis Santana-Blank, MD, Elizabeth Rodríguez-Santana, MD, Karin E. Santana-Rodríguez, BS, and Heberto Reyes, MD - Photomedicine and Laser Surgery (Publication) 4490 A broad article, but follow the references located at the original document to learn more about more applicable topics.
Objective: Set within the context of the 2015 International Year of Light and Light-Based Technologies,and of a growing and aging world population with ever-rising healthcare needs, this perspective and mini-review focuses on photobiomodulation (PBM) therapy as an emerging, cost-effective, treatment option for cancer (i.e., solid tumors) and other complex diseases, particularly, of the eye (e.g., age-related macular degeneration, diabetic retinopathy, glaucoma, retinitis pigmentosa) and the central nervous system (e.g., Alzheimer's and Parkinson's disease). Background data: Over the last decades, primary and secondary mechanisms of PBM have been revealed. These include oxygen-dependent and oxygen-independent structural and functional action pathways. Signal and target characteristics determine biological outcome, which is optimal (or even positive) only within a given set of parameters. Methods: This study was a perspective and nonsystematic literature mini-review. Results: Studies support what we describe as a paradigm shift or “quantum leap” in the understanding and use of light and its interaction with water and other relevant photo-cceptors to restore physiologic function. Conclusions: Based on existing evidence, it is argued that PBM therapy can raise the standard of care and improve the quality of life of patients for a fraction of the cost of many current approaches. PBM therapy can, therefore,benefit large, vulnerable population groups, including the elderly and the poor, whilehaving a major impact on medical practice and public finances.
The United Nations declared 2015 to be the International Year of Light and Light-Based Technologies (IYL 2015) in recognition of the vital role of light-based systems in our daily lives, and their growing importance to meeting the world's challenges in areas as diverse as energy, education, telecommunication, agriculture, and health.1 Although our perception of light is often limited to the visible band of the electromagnetic (EM) spectrum,2 both lower and shorter wavelengths are increasingly used in new medical technologies3 including soft, injectable, and bioresorbable electronics.4 Described as an imperative cross-cutting discipline of in the twenty-first century, light science has already revolutionized the physical sciences and industry. The control of light at the nanoscale has unveiled a plethora of phenomena, leading to powerful new applications and setting high expectations for years to come.5 In particular, light's ability to control materials and transport coded signals forms the bases for many new photonic devices and systems, wherein photons act as tailor-made EM energy packets that can perform various functions.
Here, we describe a paradigm shift or “quantum leap” in the understanding and use of light and its interaction with water and other relevant photoacceptors to control biologic function in medicine through photobiomodulation (PBM) therapy. We propose that progress will lead to the imminent inception of PBM therapy as a mainstream treatment for multiple complex diseases, including solid tumors, as well as neurodegenerative diseases (NDs) of the eye and central nervous system (CNS)6–10 (Fig. 1). PBM therapy can raise the standard of care and improve the quality of life of patients at a fraction of the cost of many current approaches. Thus, a “quantum leap” in PBM therapy will benefit large and vulnerable population groups, including the elderly and the poor, while having a major impact on medical practice and public finances.11 This is particularly important because the high price of drug therapies, which can reach hundreds of thousands of dollars per year,12 as well as a growing and aging world population, are putting a severe strain on family and public finances around the world.13
Flow chart illustrating fields of light-based technologies, highlighting photobiomodulation (PBM) therapy applied to complex diseases as a quantum leap in medical therapeutics.
Origin, Trajectory and Myriad Relationships in PBM's “Quantum Leap” in Medicine
Concurrent with progress in PBM therapy, a long history of discoveries has put medicine at the brink of a revolution in the use of light–water interactions for the treatment of complex diseases.7,8,10,14 Long ago, Albert Szent-Gyorgyi postulated that water was at the core of energy transfer in biological systems (i.e., quantum biology), and that that explained how energy from biomolecules could be translated into free energy for cells.15–17 Ling further elaborated on the physical state of water in living cells,18 and proposed on theoretical grounds that ordered layers of water could extend infinitely under ideal conditions.19,20Later, Huber proposed a structural basis of light energy and electron transfer in biology.21 More recently, Zewail and others showed that, with rapid laser techniques, it is possible to “see” how atoms in a molecule move during a chemical reaction.22 Light science has now reached microscales at the limit of recordable physical observation (e.g., resonant intermolecular transfer of vibrational energy in water at −100 fs)23,24showing, for example, the memory of persistent correlations in water structures within 50 fs, which is important in stabilizing biological systems.25 These and other tremendous achievements have changed our view of water, from a merely passive medium to an integral active player in the physiology of life, and have opened the gates to both direct measurement and control of physiological processes via light–water interaction.
In 2016, PBM therapy will be added to the MeSH database as an entry term for records spanning five decades of research.26 As argued by Anders et al., this is a key step, as it distinguishes PBM therapy from light-based devices used for heating of tissues, such as near infrared (NIR) lamps or other applications that rely on thermal effects for all or part of their mechanisms of action.26 In contrast, PBM therapy employs low-level monochromatic or quasimonochromatic light, currently from visible blue (∼400 nm) to far-infrared (FIR ∼3200 nm), to induce nonthermal (≤0.01°C) photochemical and photophysical effects. Nonlinear processes through which PBM therapy can stimulate or inhibit; that is, modulate, physiological activity depend upon signal-to-noise rate and target cell/tissue parameters.27–29 Thus, signal and target characteristics determine biological outcome, which is optimal (or even positive) only within a narrow set of parameters.13
Over the last decades, primary and secondary mechanisms of PBM at the tissue, cellular, and molecular levels have been revealed. These include two major structural and functional action pathways. The first, or classic, action pathway relates to oxygen-dependent mechanisms operated by oxidation-reduction enzymes of the respiratory chain, particularly cytochrome c oxidase (CcO), which is partly responsible for light energy absorption and transfer to cells and tissues.30 This pathway is associated to cofactors, pigments, metals, and proteins that act as key redox centers within the body's bioenergetic rack mechanism described by Huber.21 Nitric oxide (NO), as a first-level player, also has an activation and modulation role in the oxygen-dependent pathway.31–33
The second, or oxygen-independent, action pathway centers on the vital role of water not only as the prevalent medium of life but as an active molecule, capable of absorbing radiant energy (e.g., IR light) and transporting/transducing it along extended biological surfaces, from bulk water to confined water in nanoscopic tissue and cell spaces. Light–water dynamics precede/coexist with the classic oxygen-dependent action pathway and complement and facilitate energy transfer for increased adenosine triphosphate (ATP) production.29,34,35 As a point of comparison, correlated internal electron- and proton-transfer reactions have been tracked in real time into the oxidized enzyme (CcO), revealing an overall real time of 3.46 ms.36 This relay is slower by several orders of magnitude than total energy transport through water dynamics from bulk liquid water to confined spaces.34
Oxygen-independent light–water interactions may further power and modulate molecular signaling pathways and gene transcription factors via multiple nonmetabolic pathways.10,35 For examle, the energy of the drive force wave of an infrared pulsed laser device (IPLD) used in our group's previous studies (NIR 0.27 eV) is within the range of the strength of hydrogen bonds,29,37 and the IPLD carrier wave oscillates at a frequency (3x 10e6 Hz) that enters in vibrational resonance with the rate of electron transfer through the DNA double helix.29,37 Theoretical evidence suggests that these wave properties promote the activation of open state dynamics,38,39 allowing the activation of complex chaotic dynamics as well as the regulation of DNA replication and transcription, because the existence of open states in one place of the chain can influence the dynamics of other distant open states.29,34,35 Resulting effects match reported reductions in the frequency of chromosome aberrations induced by that low-energy laser irradiation,40 as well as theoretical,38,39 experimental,27,28 and clinical studies.41–48 These and other oxygen-independent PBM effects are channeled through metabolic control levels to regulate the energy-dependent path from the genotype to the phenotype.49,50
Light–Water Interactions and the Quantum Leap in PBM
We propose that the key to understanding and controlling the biophysics and biochemistry of higher-order organisms stems from their dual aqueous and energy-dependent nature. Water represents ∼70% by mass of an adult human body, or nearly 99% of total molecules by number, given water's low molecular weight. In addition, high-order organisms, including humans, can be represented as complex electrochemical (semiconducting) systems that comprise a vast array of energy-sensitive materials and machinery, such as ion pumps (e.g., chemically driven electron pumping through molecular wires, such as the D pathway in CcO),34 molecular motors (e.g., ATP synthase and Brownian biomotors), transistors-capacitors (e.g., cell membrane), liquid crystals (e.g., membrane structure), and rechargeable electrolytic biological batteries (e.g., hydrophilic interface in cells/tissues). Life system's double nature, whose two main structural and functional pillars are energy and water joined to biomolecules, has, therefore, tremendous consequences for life and health.
Water's permittivity, calculated considering the system as a plane capacitor, is generally high. Therefore, radiant energy can penetrate and be absorbed by tissues to provide powerful tools in medicine.51 One example is the exclusion zone (EZ) described by Pollack.52 High-energy EZ water forms along hydrophilic surfaces (e.g., tissue interfaces) in response to radiant energy.53 Remarkably, EZ water can separate and store electrical charges, and can release up to 70% of such charges when it is perturbed, such as by injury-induced redox potentials.54 We have argued that supplied energy can power and modulate cellular work and signaling pathways, even when the metabolic energy pathway has been compromised, steering cells toward or away from programmed cell death.34 EZ water may, thus, act as an electrolytic bio-battery,35 which can efficiently and selectively transfer energy to sites expressing redox injury potentials, as found in cancer and other complex diseases, triggering reparative and regenerative mechanisms that can lead to restoring homeostasis/homeokinesis and, ultimately, health.29,34,35
Experimentally, IR energy absorption by water has been recently modeled in a porcine model, confirming that absorption depends upon fluence and wavelength. Further, the higher the concentration of water in tissues, the higher IR energy absorption will be.55 This is consistent with controlled clinical studies in solid tumors and complex ophthalmic and neurologic diseases,9,46,56 as well as molecular, biochemical, biophysical, and metabolic mechanistic support for a quantum leap in medical therapeutics based on the simple, but powerful, idea that properly tailored light can power and modulate physiologically reparative mechanisms.30,57–62
The bases of our understanding of cancer are constantly being questioned and revised, leading to new treatment goals. In a paradigm-changing editorial, Prendergast recently argued that “disorders in microenvironment and peripheral systems that control cancer might increasingly be viewed as primary rather than secondary factors in the root nature of cancer as a clinical disease.” This constitutes “a crucial and radical distinction from prevailing thought, since it implies that cancer may be a symptom of an underlying clinical disorder, rather than the root problem itself that needs to be addressed.” 6,63
Prendergast further suggested that “effective treatment of cancer may not necessarily entail understanding or addressing this complexity, but mastering the use of tissue or systemic systems that have the inherent ability to do so.” Hence, a common thread linking emerging perspectives in oncology and PBM therapy may well be the restitution of tissue homeostasis-homeokinesis via light-energy supplementation, a microenvironment effect that comprises and extends the Warburg effect previously discussed by our group.57,64–67
As far back as 1964–1966, McGuff et al. showed 64,65 that “laser energy has a selective effect on certain malignant tumors, resulting in their progressive regression and ultimate dissolution.” Following years of controversy,66,67 editorials by Karu68 and Lanzafame11,69 now stress evidence supporting the potential anticancer effects of PBM.11,68,69 New data confirm that PBM under certain parameters is safe for use in cancer patients.60 This is in accord with clinical results from our group using the abovementioned proof of concept IPLD.4,44
A phase I trial in patients with advanced neoplasias demonstrated that the IPLD studied was safe for clinical use and improved performance status and quality of life.41 Antitumor activity was observed in 88.23% of patients with 10 years of follow-up.41
In that series, T2-weighted MRI data showed increased water content of tumor heterogeneities42,44 preceding tumor-volume reduction and a therapeutic anticancer effect.42,44 Structural, kinetic, and thermodynamic implications of these changes in water dynamics have been analyzed at the tissue, cell, and interstitial levels.27 In conjunction, selective activation of programmed cellular death [i.e., apoptosis, necrosis, and anoikis (cell death by loss of cell adhesion)] and cytomorphologic modification (e.g., reduced size, increased roundness, increased vacuoles) were documented in neoplastic cells, but not in peripheral tissues.8,42 Modulation of cluster of differentiation (CD)4 CD45RA+, CD25 activated, tumor necrosis factor alpha (TNF-α), and soluble interleukin (IL)-2 receptor (sIL-2R) was further documented.43These hallmark results, supported by independent data,70–72 demonstrate that PBM therapy can modulate antitumor effects,6,8 in sharp contrast with long-held views.45,73,74 This evidence is also consistent with growing experimental and clinical reports from multiple other authors.60,75–82
PBM and Ophthalmic and Neurodegenerative Disorders
Recent evidence underscores common mechanisms between cancer and NDs of the eye and CNS. Research suggests that oxidative proteome damage may be the most likely cause of aging and age-related maladies such as cancer and other complex diseases, including NDs.83 Findings also show “common mechanisms of onset,” with a focus on genes such as DJ-1 and Myc-Modulator 1 (MM-1) and signaling pathways that contribute to the onset and pathogenesis of cancer and NDs such as retinitis pigmentosa (RP), Parkinson disease (PD), and cerebellar atrophy.”84 Finally, both disease groups are profoundly energetic in nature, featuring prominent deterioration of metabolic energy pathways.10
External light energy supplementation has been shown to generate neuroprotective, vasoprotective, baroprotective, immunomodulatory, and regenerative effects (Fig. 2). 47 We have documented that such effects may be activated and modulated locally and/or remotely via oxygen-dependent and oxygen-independent pathways that can encompass extended biologic surfaces and may even reach avascular eye tissues (i.e., cornea, lens, aqueous humor, and vitreous) noninvasively. Although a full elucidation of involved mechanisms escapes the scope of this perspective and mini-review, a very brief discussion of results from multiple authors is given subsequently.
Electromagnetic (light) energy supplementation based on water–light interactions. Upper left side shows classic oxygen (O2) dependent pathways by which light energy generates adenosine triphosphate (ATP)/ guanosine-5′-triphosphate (GTP) and other high-energy molecules. Upper right side shows O2 independent pathways by which photoinduced, nonlinear, oscillations in water provide energy for cellular work, signaling, and gene transcription. Top center shows interfacial exclusion zone (EZ) water, which acts as a selective rechargeable electrolytic bio-battery. Together, these pathways activate and modulate physiologically reparative mechanisms which, at appropriate irradiation parameters, can generate neuroprotective, vasoprotective, baroprotective, immunomodulator, and regenerative effects locally and remotely, promoting homeostasis/homeokinesis through the coupling and synchronization of biophysical, biochemical, biomechanical, and hydrodynamic oscillators, as guided by the second law of thermodynamics. Arrows point to the sequence and direction of events. (Updated from reference 47. Authors retained copyright.)
PBM has shown promise in the treatment of diabetic retinopathy (DR),85,86 age-related macular degeneration (AMD),46 glaucoma,47 RP,87 Stargardt disease,88 Leber's hereditary optic neuropathy,89 Alzheimer's disease (AD), and PD, 90,91 among other conditions.89 Strikingly, although each of these NDs has different etiologies and pathogeneses, “they frequently induce a set of cell signals that lead to well-established and similar morphological and functional changes, including programmed cell death. Furthermore, oxidative stress, activation of apoptotic pathways and inflammatory response, are common features in all these diseases.”92
Remarkably, PBM can modulate apoptosis as well as necrosis.42,45,47 PBM can also be both pro-oxidant in the short term, but antioxidant in the long term,93 thus modulating reactive oxygen species (ROS) generation. We also found clinical evidence of immune regulatory effects over inflammation during treatment of solid tumors with the IPLD, a NIR diode laser pulsed at a frequency of 3 MHz.43 These results are in agreement with the regulating role of the vagal reflex on the inflammatory reflex reported by Tracey, using an electronic device that stimulated nerves to treat inflammation.71,72
In addition, PBM has been shown to protect against retinal dysfunction and photoreceptor cell death in rodent models of retinal injury and retinal degeneration.94 PBM has been further reported to attenuate oxidative stress and inflammation in primary astrocytes induced by amyloid β peptide (Aβ),95 and to reduce Aβ-induced apoptosis,96 which is thought to play a major role in AD. Nevertheless, it has been argued that red to NIR light cannot be transmitted through the scalp to the brain more than a few centimeters,97 which makes it nearly impossible to noninvasively treat AD with PBM 98 using conventional (direct) delivery systems/methods. Similarly, although an absence of adverse effects from 670 and 830 nm PBM applied to the retina in Sprague Dawley albino rats has been reported,94 extreme care must be taken to avoid photodamage of the eye99 from direct PBM procedures.
Conversely, we published an interventional case report of a patient with bilateral geographic atrophic AMD (gaAMD) and associated neurologic disease treated noninvasively, indirectly, and at a distance (i.e., remotely) from ocular structures and the CNS with the above-referenced IPLD/photo-infrared pulsed bio-modulation (PIPBM).46 Results showed neurologic improvement, transitory color vision, enhanced visual acuity, full-field electroretinogram (ERG) modifications toward a normal rhythm, drusen mobilization, decreased lens opacity, and lower intraocular pressure (IOP), in accord with a retrospective noncomparative data analysis from the phase I trial of patients with advanced cancer treated with the IPLD,41 which showed statistically significant evidence of a therapeutic hypotensor effect over IOP,47 and they are consistent with the positive neurological evolution of two trial patients.
Moreover, although trial participants did not develop media opacity, one pre-existing incipient cataract in the right eye of a patient (transitional meningioma) became denser and slightly smaller 3 months post-treatment, and remained unchanged 1 year post-treatment. The left eye lens of the same patient was unaffected. Although the finding could be part of the natural history of the cataract, we stressed that possible deterministic effects related to the initial metabolic or biochemical state of lens opacities should be studied.41
In accordance with the what was described, a robust body of evidence suggests that protein misfolding, insolubility, and aggregation are at the root of both cataracts and other diseases including AD, PD, and Huntington's disease,100 and that external EM energy (light) supplementation can have reparative effect on protein misfolding, activating and modulating metabolic control levels of protein folding/unfolding.10,34In addition, PBM effects on targets such as heat shock proteins (α crystalline), enzymes of the antioxidative system, Na+-K+-ATPase, Ca +2-ATPase, aquaporins (AQPs), and ion pumps have been referred to as part of mechanisms that could have influenced the response observed in the lens on the cases studied.46 We further proposed that, among other effects, PBM can stimulate and/or substitute ATP production via water dynamics, which is vital for the activation and inactivation kinetics in phototransduction.46 PBM can also affect the synthesis of molecules in a liquid crystalline (LC) state (e.g., self-assembly of lipids, water, and other biomolecules such as proteins and sterols, which are sensitive to temperature and/or electric fields) If confirmed, the latter may have multidisciplinary applications in medicine and biology in areas such as photovision, in which LCs are essential functional components.28
A first rapid communication referring to the retina and optic nerve additionally showed first evidence of EZ water as a selective rechargeable bio-battery applicable to PBM, suggesting a new understanding of the eye's energetic environment, which may have deep implications in ocular physiology as well as in the pathophysiology, diagnosis, and treatment of blinding diseases using light-based therapies.48 Therefore, as a promising alternative to drug therapies,101 or in combination with other treatments, PBM therapy may be developed into a viable therapeutic approach with multidisciplinary applications in ophthalmology and neuroscience,46 inducing and modulating physiologically reparative and regenerative effects that can favor homeostasis/homeokinesis27–29 through the coupling and synchronization of biophysical, biochemical, biomechanical, and hydrodynamic oscillators, as guided by thermodynamics.
At the 2015 American Society of Clinical Oncology (ASCO) annual meeting, Dr. Leonard Saltz, chief of gastrointestinal oncology at Memorial Sloan Kettering Cancer Center, discussed the high cost of cancer drugs. He argued that “the unsustainably high prices of cancer drugs is a big problem, and it's our problem,” citing as examples the cost of nivolumab ($28.78/mg) and ipilimumab ($157.46/mg), which is “approximately 4000 times the cost of gold.”102 Previously, >100 oncologists had protested the high price of cancer drugs, also calling them economically “unsustainable.” They noted that, of 12 cancer drugs approved in 2012, 11 were priced > $100,000 per year,103 with multiple drugs often being required for extended periods. Such high prices and their impact on families, governments, and society at large are leading some to propose that cost should be considered a “financial toxicity” to be assessed with other toxicities when treatments are considered by doctors and patients.104 In contrast, although it has been estimated the cost of developing new drug therapies can run up to USD $1.3–$1.7 billion,105,106 the development cost of new photonics devices can be substantially lower, which can lower therapy costs and increase treatment availability. For the same reasons, PBM can also offer a noninvasive and cost-effective therapeutic option for patients with NDs of the retina, brain, and beyond.56, 85
The celebration of the IYL 2015 by the United Nations1 is a fitting time to announce what we describe here as a “quantum leap” in PBM therapy. It is also a good opportunity to ensure that policy makers and the medical community become aware of and embrace the immense potential of light-based medical technologies, especially PBM therapy, as an emerging treatment option for cancer and other complex diseases.107 Although not all tissues respond to PBM therapy,69in vitro and in vivo xenografts and evidence from clinical studies does suggest that it is time to begin considering PBM therapy as a potential drug equivalent.11,108 In addition, PBM therapy may have minimal or no adverse effects, improve quality of life and functional status and raise the current standard of care for many cancer patients when used alone or in combination with other therapies.9 PBM therapy further represents a novel hope for the treatment of numerous eye and neurologic diseases. And as stated, PBM may be developed at a lower cost than many current treatments,8,10 which can help meet the healthcare needs of an increasing and aging world population. As such, this perspective and mini-review focuses on the large potential tangible contributions of light-based therapies for large demographic segments of the population, such as aging “baby boomers” who are expected to face a higher incidence of diseases such as cancer, AMD, DR, glaucoma, RP, AD, and PD, as well as other neurologic diseases in the next 15 years. In light of the growing costs of drugs and their impact on developed and developing countries, we propose that PBM therapy may offer a novel, safe, and effective therapy choice that would be more accessible to large vulnerable groups, such as the poor and the elderly.
Concurrently with the United Nations' declaration of 2015 as the year of light and light-based technologies, PBM therapy stands at the brink of delivering a new generation of treatments for complex diseases. New PBM therapies will preserve quality of life and raise standard of care in an efficient and cost-efficient manner. This will particularly benefit the most vulnerable demographic sectors, such as the elderly and the poor, and reduce the strain of growing healthcare costs in both industrialized and developing countries. We propose that such developments and their imminent impact represent a paradigm shift or “quantum leap” in PBM therapy and medicine at large.
We thank Jesús Alberto Santana-Rodríguez for reviewing and editing this article, and Luis Rafael Santana-Rodríguez for design and technical support. This study was supported by Fundalas, Foundation for Interdisciplinary Research and Development.
This book covers an astonishing amount of information in its near thousand pages, everthing from basic laser physics to dental, and veteranary useage. Here are some of its contents:
Basic Laser Physics
physics
energy
radiation
wavelength and frequency
photon energy
the elecromagnetic spectrum
the optical reigon
radiation risks
can electromagnetic radiation cause cancer
protective mechanisms
light
the optical spectrum
light sources
various sources of radiation
natural sources of radiation
man-made light sources
the light emmiting diode (LED)
flash lamps
the laser
laser design
practical lasers
the properties of laser light coherence
interference
laser beam characteristics
polarisation
output power
continuous and pulsed lasers
the peak power value
average power output
power density
light distribution
beam divergence
collimation
risk of eye injury
decisive factors in the risk of eye injury
the laser instrument
properties of some laser types
description of common surgical laser types
the CO2 laser (carbon dioxide laser)
carbon dioxide lasers in surgery
carbon dioxide lasers in dental applications
the Nd:YAG laser
Nd:YAG lasers in surgery
Nd:YAG lasers in dentistry
erbium lasers in dentistry
"strong" diode lasers in dentistry
the KTP laser
Q-switching
Theraputic Lasers
the first generation 1975-85
the second generation 1985-95
the third generation 1995-2005
the fourth generation 2005 and onwards
what is a good laser therapy instrument
the basic instrument
sales tricks
high power-low power
laser or LED
high or low price
penetration of light into tissue
"a story of a young scientist"
the wavelength
how deep does light penetrate into tissue?
Biostimulation
history
a few words on mechanisms
photoreceptors
what parameters to use
laser parameters
whitch wavelength?
output power
average output power
power density
energy density
the dose
treatment dose
calculation of doses
dose ranges
calculation of treatment time for a desired dose
"reay reckoner"
dose per point
pulsed or continuous light
pulse repetition rate (PRP)
patient parameters
treatment area
treatment intervals
pre- or postoperative treatment
treatment method parameters
local treatment
shallow problems
deeper problems
treating inside the body
systemic treatments
acccupuncture
trigger points
spinal processes
dermatome
blood irradiation
irradiation of lymph nodes
irradiation of ganglions
combo treatment
interaction with medication
other considerations
what about collimation?
depth of penetration, greatest active depth
factors that reduce penetration
tissue compression
how deep does the light penetrate?
laser light irradiation through clothes
the importance of tissue and cell condition
the importance of ambient light
in vitro/ in vivo
laser therapy with high output lasers
laser therapy with carbon dioxide lasers
laser therapy with Nd:YAG lasers
laser therapy with ruby lasers
laser therapy with Er:YAG lasers
laser therapy with surgical diode lasers
risks and side effects
the importance of correct diagnose
cancer
cytogentic effects?
a false picture of health
tiredness
pain reaction
do high doses of laser therapy damage tissue?
is it only an effect of temperature?
protection against radiation injury
how to measure effects of laser therapy
thermography
magnetic resonance imaging
high resolution digitized ultrasound B-scan
tensile strength
other objective methods
does it have to be a laser?
FDA (Food and Drug Administration)
how well documented?
confused?
the funding research
as time goes by
Medical indications
who and what can be treated?
acne
allergy
antibiotic resistance
arteriosclerosis
arthritis
asthma
blood preservation
blood pressure
bone regeneration
burning mouth syndrome
cancer
cardiac conditions
carpal tunnel syndrome
cerebral palsy
crural and venous ulcers
delayed onset muscular soreness (DOMS)
depression, psychosomatic problems
diabetes
duodenal/gastric ulcer
epicondylitis
erythema multiform major
fibrositis/fribomyalgia
headache/migraine
heamorrhoids
herpes simplex
immune system modulation
inflammation
inner ear conditions
laryngitis
lichen
low back pain
mastitis
microcirculation
morbus sluder
mucositis
muscle regeneration
mycosis
nerve conduction
nerve regeneration and function
oedema
ophthalmic problems
pain
periostitis
plantar fasciitis
salivary glands
sinuitis
spinal cord injuries
snake bites
sports injuries
stem cells
stroke, irradiation of the brain
tendinopathies
tinnitus, vertigo, meniere's disease
tonsillitis
trigeminal neuralgia
thrombophlebitis
tuberculosis
urology
warts
wiplash-assosiated dissorders
vitiligo
womens' health
wound healing
zoster
idications in the pipeline
alzheimer's disease
botox failures
cellulites
cholesterol reduction
complex reigonal pain syndrom (CRPS)
eczema
erectile dysfunction
familiar amyotrophic lateral sclerosis (FALS)
glomerulonephritis
obesity
orofacial granulomatosis
Parkinson's disease
post-mestrual stress
pemphigus vulgaris
sleeping disorders
withdrawal periods
wrinkles
consumer lasers
Dental LPT
the dental laser literature
on which patients can LPT be used?
dental indications
alveolitis
anaesthetics
aphthae
bleeding
bisphosphonate related osteonecrosis of the jaw
caries
dentitio dificilis (pericoronitis)
endodontics
extraction
gingivitus
herpes zoster
hypersensitive dentine
implantology
leukoplakia
lingua geographica (glossitis)
lip wounds
nausea
nerve injury
orthodontics
mild dental pain
paediatric dental treatment
periodontics
prosthetics
root fractures
secondary dentine formations
temperature caveats
toemporo-mandibular disorders (TMD)
TMD and endodontics
other dental laser applications
dental pohoto dynamic therapy
composite curing
deminerallisation
tooth bleaching
caries detection
lasers as a diagnostic tool
case reports
Non Coherent Light Sources
Veterinary Use
case reports
Contra Idications
pacemakers
pregnancy
epilepsy
thyroid gland
children
cancer
haemophilia
irradiation of the brain
radiation therapy patients
diabetes
tatoos
light sensitivity
Coherence
the role of coherence in laser phototherapy
itroduction
summary
Dose and Intensity
basics about energy
output power
power density
the laser beam
the laser probe
pulsed lasers
energy density
treatment dose
the dose does not demend on the intensity
dose per point
more about treatment technique
The Mechanisms
are biostimulative effects laser specific?
is it possible to prove that laser therapy doesn't work?
comparisons between coherent and non-coherent light
what is the importance of the length of coherence
hode's hamburger
hode's big burger
abrahamson's apple
moonlight
how deep does light penetrate tissue?
bright light phototherapy
similarities and differences
possible primary mechanisms
polarisation effects
what characterises the light in a laser speckle
porphyrins and polarised light
cell cultures and tissue have different optical properties
tthe effect of heat development in the tissue
macroscopic heating
the microscopic heat effect
mechanical forces
excitation effects
primary reactions due to excitation
secondary reactions due to cell signaling
flourescence-luminescence
multi-photon effects
llasting effects in tissue
non-linear optical effects
opto-acoustic waves
secondary mechanisms
effects on pain
effects on blood circulation
stimulatory and regulatory mechanisms
effects on the immune system
other interesting possibilities
summary of mechanisms
diagnostics with therapeutic lasers
photodynamic therapy - PDT
other medical uses of lasers
A Guide for Scientific Work
methodology of a trial
parameters
technical parameters
treatment parameters
medical parameters
closer description of the technical parameters
name of instrument (producer)
laser type and wavelength
laser beam characteristics
number of sources
beam delivery system
output power
power density at probe aperture
calibration of the instrument
closer description of the treatment parameters
treatment area
dose: energy density
dose per treatment and total dose
intensity: power density
treatment method
treatment distance (spot size), type of movement, scanning
sites of treatment
number of treatment sessions
frequency of treatment sessions
closer description of the medical parameters
description of the problem to be treated
patients (number, age, sex)
exclusion criteria
inclusion criteria
condition of patient
pre-, parallel-, or post-medication
treated with other methods before
drop-out rates
follow up
outcome measures
statistical analysis
economy
gallium-alluminium and all that
recommendations of WALT - the world assosiation for laser therapy
The Laser Phototherapy Literature
the importance of reporting all laser parameters - even in the abstract
diclofenac, dexamethasone or laser phototherapy?
another pithole in LPT research
database of abstracts of reviews of effects (DARE)
A Practical Handbook Laser Acupuncture Successful Treatment Concepts
Volkmar Kreisel and Michael Weber - 2012 (Book) 4330 This book is our top recommendation for any acupuncture style cold laser treatment protocols. It is beautifully written and illustrated.
dHae In Lee Sae, Won Lee Nam Gyun Kim Kyoung Jun Park Byung Tae Choi Yong Shin Hwa Kyoung Shin - Wiley-VCH Verlag GmbH & Co. 06 February 2017 (Publication) 4481
Use of photostimulation including low?level light emitting diode (LED) therapy has broadened greatly in recent years because it is compact, portable, and easy to use. Here, the effects of photostimulation by LED (610 nm) therapy on ischemic brain damage was investigated in mice in which treatment started after a stroke in a clinically relevant setting. The mice underwent LED therapy (20 min) twice a day for 3 days, commencing at 4 hours post?ischemia. LED therapy group generated a significantly smaller infarct size and improvements in neurological function based on neurologic test score. LED therapy profoundly reduced neuroinflammatory responses including neutrophil infiltration and microglia activation in the ischemic cortex. LED therapy also decreased cell death and attenuated the NLRP3 inflammasome, in accordance with down?regulation of pro?inflammatory cytokines IL?1β and IL?18 in the ischemic brain. Moreover, the mice with post?ischemic LED therapy showed suppressed TLR?2 levels, MAPK signaling and NF?kB activation. These findings suggest that by suppressing the inflammasome, LED therapy can attenuate neuroinflammatory responses and tissue damage following ischemic stroke. Therapeutic interventions targeting the inflammasome via photostimulation with LED may be a novel approach to ameliorate brain injury following ischemic stroke.
Effect of post?ischemic low?level light emitting diode therapy (LED?T) on infarct reduction was mediated by inflammasome suppression.
Introduction
Ischemic stroke, a cerebrovascular insult, is the most common cause of physical disabilities worldwide. However, the only FDA approved treatment is tissue plasminogen activator that must be administered up to 4.5 hours after stroke onset 1. Therefore, identifying new stroke therapeutics would address a significant unmet medical need. Ischemic stroke initiates a complex cascade of events that leads to focal brain damage, and in which inflammation plays a significant role 2. The inflammatory response includes activation of resident microglia and production of pro?inflammatory cytokines 3, followed rapidly by infiltration and accumulation of neutrophils and monocytes/macrophages in microvessels and ischemic cerebral parenchyma 4.
Inflammatory mechanisms that contribute to cell death in cerebral ischemia are mediated by a multi?protein complex called the inflammasome 5-9. The key component is NOD?like receptor pyridine domain?containing (NLRP) protein, which initiates inflammasome activation when bound by its ligand. More specifically, the NLRP1 and NLRP3 inflammasomes are cytosolic complexes containing NLRP1 or NLRP3 receptor protein, ASC (apoptosis?associated speck?like protein containing a caspase recruitment domain), X?linked inhibitor of apoptosis (XIAP), precursor caspase?1 and/or precursor caspase?11 10. First, toll?like receptors (TLRs) trigger mitogen activated protein kinase (MAPK) signaling pathways and nuclear factor kappa?B (NF?kB) activation, which regulate NLRP3 expression 11-13 and induce formation of the inflammasome. Its activation then cleaves pro?caspase?1 into the bioactive form, which then induces production of active IL?1β and IL?18; ultimately, this induces pyroptosis, a type of inflammatory cell death 5-9, 14, 15. Therefore, targeting components in the inflammasome pathways may offer a new therapeutic strategy for the treatment of ischemic stroke.
Recently low?level light therapy has gained attraction in treating neurological and psychological disorders because it is relatively cheap, non?invasive, and safe 16-20. Low?level light therapy has been used neurotherapeutically because it can penetrate the scalp and skull 21. In addition, low?level light therapy can modulate a wide range of cellular processes via absorption of light energy via chromophores or photoreceptors in the mitochondria 22. The photochemistry hypothesis is a widely accepted to explain the induction of photobiological effects such as increasing energy in the form of ATP, generating reactive oxygen species (ROS) and nitric oxide, and modification of intracellular organelle membrane activity; these then lead to activation of downstream signaling pathways and transcription factors 23, 24. Transcranial near?infrared light therapy was shown to reduce ischemic brain damage in rabbit acute ischemic stroke 25. Light therapy (710 nm) showed neuroprotection in rat experimental stroke models 26, 27, and has shown clinical promise when tissue regeneration and prevention of tissue damage are required 23. Furthermore, low?level laser light (800 nm) improves cognitive deficits and modulates neuroinflammation after traumatic brain injury 28, 29, and low?level laser therapy (632.8 nm) suppresses microglia activation in BV2 microglial cells 29.
While the use of low?level light therapy mostly involves red and near?infrared light, low?power light emitting diode (LED) using visible light is attractive because LEDs are safer, generating negligible heat at the targeted tissue surface. In addition, LEDs are more affordable, compact/portable, and easier to use. Therefore, we investigated whether acute LED therapy using visible light (orange; 610 nm; see Figure 1 for details on the apparatus) could suppress ischemic brain damage in a focal cerebral ischemia mouse model, using clinically relevant post?stroke parameters.
Experimental scheme of the low?level light emitting diode (LED) therapy. (A) The technical characteristics of the skin?adherent low?level light emitting diode probe. (B) The mice underwent LED therapy (20 min) twice a day for 3 days commencing at 4 h post?ischemia. The control group was kept under isoflurane anesthesia for 20 min without LED application.
Materials and methods
General surgical preparation
All animal experiments were conducted in accordance with the guidelines of the Pusan National University?Institutional Animal Care and Use Committee (PNU?IACUC) on their ethical procedures and scientific care, and were approved by the PNU?IACUC in Pusan National University (Approval Number PNU?2014?0646). Male mice (C57BL/6J, 20–25 g) were housed under diurnal lighting conditions and allowed food and tap water ad libitum. Anesthesia was achieved by face mask?delivered isoflurane (2% induction and 1.5% maintenance, in 80% N2O and 20% O2). Rectal temperature was maintained at 36.5–37.5 °C using a Panlab thermostatically controlled heating mat (Harvard Apparatus, Holliston, MA).
Low?level light emitting diodes (LED) therapy
A skin?adherent LED probe (Color Seven Co., Seoul, Korea) was used for LED therapy with the following technical characteristics: peak wavelength, 610 nm (orange color); power intensity, 1.7 mW/cm2; energy density, 2.0 J/cm2 (Figure 1A). Light stimulation was applied by placing the probes (spot size, 4?mm diameter) onto the skin via double?sided tape at two locations on the head (the right midpoint of the parietal bone and the posterior midline of the seventh cervical vertebra) concurrently (Figure 1B). The mice underwent LED therapy (20 min) twice a day for 3 days, commencing at 4 h after the ischemic insult. The control group was kept under isoflurane anesthesia for 20 min without LED (Figure 1B). Experimental drugs including a TLR2 agonist (Pam2CSK4; 50 µg/kg, Invivogen, San Diego, CA) 30, NLRP3 agonist (MSU crystals; 10 mg/kg, Invivogen) 31, and NLRP3 antagonist (MCC950; 10 mg/kg, Sigma, St. Louis, MO) 32 were intraperitoneally administered to mice 30 min before LED therapy. Control mice were administered PBS.
Focal cerebral ischemia
Focal cerebral ischemia was induced by photothrombosis of the cortical microvessels 33. The advantages of this model are simple animal preparation, no craniotomy or mechanical manipulation of cerebral blood vessels or parenchyma, and easily reproducible lesion size and location. Briefly, photochemical dye Rose Bengal (Sigma?Aldrich, St. Louis, MO; 0.1 ml of a 10 mg/ml solution in sterile saline) was injected intraperitoneally so that it entered the blood stream 5 min before illumination. When brain is illuminated by a Cold?light source CL 6000 LED (Carl Zeiss, Jena, Germany), the dye becomes activated and induces endothelial damage with platelet activation and thrombosis, resulting in local blood flow interruption 34. The mice were placed in a stereotaxic frame (David Kopf Instruments, Tujunga, CA) for illumination, the skull was exposed, and bregma and lambda identified. A fiber optic bundle of a cold light source with a 4 mm aperture was centered 2.4 mm laterally from the bregma using a micromanipulator located over the sensorimotor cortex. The brain was illuminated for 15 min, the surgical wound was sutured, and the mice were allowed to recover from anesthesia (Figure 1B).
Infarct volume
Mice were deeply anesthetized with sodium thiopental 72 h after ischemic insults, and the brains were removed. The cerebral infarct size was determined on 2,3,5?triphenyltetrazolium chloride (TTC)?stained, 2?mm?thick brain sections. Infarction areas were quantified using the iSolution full image analysis software (Image & Microscope Technology, Vancouver, Canada). To account for and eliminate the effects of swelling/edema, the infarction volume was calculated using an indirect measurement in which the volumes of each section were summed according to the following formula: contralateral hemisphere (mm3) – undamaged ipsilateral hemisphere (mm3).
Neurological score
Neurological deficit was scored in each mouse at 72 h after ischemic insult in a blinded fashion according to the following graded scoring system: 0 = no deficit; 1 = forelimb weakness and torso turning to the ipsilateral side when held by the tail; 2 = circling to the affected side; 3 = unable to bear weight on the affected side; and 4 = no spontaneous locomotor activity or barrel rolling 35.
Western blotting
Mice were deeply anesthetized with sodium thiopental 72 h after the induction of ischemia, and then perfused transcardially with cold PBS. Brain cortices were subsequently collected and total protein was isolated according to the standard methods. Samples were separated by 12% sodium dodecyl sulfate?polyacrylamide gel electrophoresis, and transferred onto a polyvinylidene difluoride (PVDF) membrane (Amersham Biosciences, Piscataway, NJ). Immunoblot analysis was performed with the specific primary antibodies followed by secondary antibody conjugated with horseradish peroxidase: TLR?2 (1 : 1000; sc?16237), TLR?4 (1 : 1000; sc?293072), NF?κB p65 (1 : 1000; sc?109), ASC (1 : 1000; sc?22514?R), precursor IL?1β (1 : 500; sc?7884), mature IL?1β (1 : 500, sc?7884), precursor IL?18 (1 : 500; sc?7954), mature IL?18 (1 : 500; sc?7954, Santa Cruz Biotechnology, Dallas, TX), p38 (1 : 1000; 9212S), p?p38 (1 : 1000; 9212S), JNK (1 : 1000; 9251S), p?JNK (1 : 1000; 9251S), ERK (1 : 1000; 4695), p?ERK (1 : 1000; 4695, Cell signaling, Danvers, MA), NLRP1 (1 : 1000; NBP1?54899), NLRP3 (1 : 1000; NBP1?77080), XIAP (1 : 1000; NB100?56183), cleaved caspase?1 (1 : 500; NBP1?45433), pro?caspase?1 (1 : 500; NBP1?45433), cleaved caspase?11 (1 : 500; NBP1?45453), pro?caspase?11 (1 : 500; NBP1?45453, Novus Biologicals, Littleton, CO), myeloperoxidase (MPO, 1 : 1000; af3667, R&D systems, Minneapolis, MN). The intensity of chemiluminescence was measured using an ImageQuant LAS 4000 apparatus (GE Healthcare Life Sciences, Uppsala, Sweden). The membrane was then stripped and incubated with anti?β?actin (1 : 2000; A5316, Sigma) or anti?Lamin B (1 : 1000; sc?3740, Santa Cruz Biotechnology) antibodies as an internal control.
TUNEL analysis and PI staining
Neuronal death was evaluated by TUNEL analysis and propidium iodide (PI) staining. Mice were perfused transcardially with cold PBS prior to processing of tissue. The frozen brains were cut to a thickness of 8 μm using a CM 3050 cryostat (Leica Microsystems, Wetzlar, Germany), and the TUNEL assay was performed using a DeadEndTM Fluorometric TUNEL System kit (Promega Corporation, Madison, WI). For PI staining, brain sections were incubated with PI (50 μg/ml). After mounting using a fluorescent mounting medium (Vector Laboratories, Inc., Burlingame, CA), images were obtained with a fluorescence microscope (Axio Imager M1, Carl Zeiss). TUNEL(+)/PI(+) cells were counted blindly from three fields per three predefined areas per three adjacent brain sections from each mouse.
Immunohistochemical staining
Seventy two hours after focal cerebral ischemia, mice were deeply anesthetized with sodium thiopental and subsequently perfused transcardially with cold PBS followed by 4% paraformaldehyde for fixation. Each mouse brain was removed and further fixed in 4% paraformaldehyde at 4 °C for 24 h, followed by cryoprotection in 30% sucrose for 72 h at 4 °C. Next, the isolated brains were frozen in an optimal cutting temperature medium for frozen tissue specimens (Sakura Finetek, Torrance, CA) and stored at –80 °C until examined. The frozen brains were cut to a thickness of 14 μm using a CM 3050 cryostat (Leica Microsystems), and the sections were pretreated with 0.1% H2O2 for 20 min, incubated with blocking buffer (CAS block; Invitrogen Corporation, Carlsbad, CA), and subsequently incubated with primary antibodies against Iba?1 (1 : 200; 019?19741, Wako, Pure Chemical Industries, Osaka, Japan) at 4 °C overnight. The sections were then incubated with biotinylated secondary antibody (1 : 500; BA?1000, Vector Laboratories, Inc.) for 2 h. After several washing, sections were incubated in an avidin?biotinylated peroxidase complex (ABC) reagent (Vectastain ABC kit, Vector Laboratories Inc.) and visualized using a diaminobenzidine (DAB) solution (Vector Laboratories Inc.). All samples were visualized using a light microscope (Carl Zeiss, Jena, Germany). For immunofluorescence staining, the brain sections were immunostained with primary antibodies against MPO (1 : 300; af3667, R&D systems), Iba?1 (1 : 200; 019?19741, Wako, Pure Chemical Industries) or CD68 (1 : 500; MCA1957GA, AbD Serotec, Oxford, UK) at 4 °C overnight. The samples were incubated with FITC? (1 : 500; FI?1000, FI?5000) or Texas Red?conjugated secondary antibodies (1 : 500; TI?9400, Vector Laboratories, Inc.) for 2 h in the dark. The images of each section were captured with a fluorescence microscope (Axio Imager M1, Carl Zeiss) and morphological analysis and quantification of positive cells was conducted using the iSolution analysis software (Image & Microscope Technology). For quantification of positive cells, at least three randomly selected fields (0.36 mm2/field) in the peri?infarct area were examined and averaged. The MPO(+) or Iba?1(+)/CD68(+) cells from three fields per three adjacent brain sections from each mouse were counted.
Data analysis
Quantification of band intensity was performed by Image J software (NIH, Bethesda, MD, USA) and normalized to the intensity of internal control. Data are expressed as the means ± the SEM. Differences between two groups were determined using the unpaired t?test; and comparing more than two groups was determined by one?way analysis of variance (ANOVA) followed by Student?Newman?Keuls test. A P < 0.05 was considered statistically significant.
Results
LED therapy reduced brain damage when administered after stroke onset
We first evaluated whether post?ischemic treatment with LED therapy could improve tissue and functional outcomes following focal cerebral ischemia (Figures 1 and 2). As shown in Figure 2A, TTC staining revealed that LED therapy significantly reduced infarct volume relative to controls when measured 72 h after ischemic brain injury (37.0 ± 5.0 mm3 vs. 58.0 ± 7.0 mm3, LED therapy and control, respectively, P < 0.05; Figure 2A and B). Thus, acute LED therapy treatment reduces the spread of ischemic damage. As with infarct volume, ischemia?induced neurological deficits were significantly attenuated in the LED?treated mice (P < 0.05; Figure 2C and Supplementary file), as measured by a scored evaluation of neurologic function (a lower score represents less deficit; see Supplementary file). Together, these findings indicated that acute post?ischemic LED therapy improved tissue?level markers of ischemic damage, and neurological function, in a focal cerebral ischemic mouse model.
Post?ischemic LED therapy improved tissue and functional outcome in a mouse model of ischemic stroke. (A, B) LED therapy (LED?T) reduced infarct volume compared with the control mice (Con). At 72 h after photothrombotic cortical ischemia, brains were removed and brain sections were sequentially obtained. Coronal brain sections (2?mm?thick) were stained with 2,3,5?triphenyltetrazolium chloride (TTC). White indicates the infarct area (A). Quantification of the infarct volume (B) was analyzed using the iSolution full image analysis software (N = 9, * P < 0.05 vs. control group). (C) LED therapy improved neurologic function after cerebral ischemia. Neurological deficit was evaluated 72 h after cerebral ischemia in a blinded fashion followed by neurological score (0 means no deficit. The lower score represents less deficit). Data are expressed as the means ± SEM (N = 9). * P < 0.05 when compared with the control group (Con).
LED therapy attenuated post?ischemic neuroinflammatory responses
We investigated whether LED therapy modulated ischemia?related neuroinflammation by immunofluorescence staining and western blotting for myeloperoxidase (MPO; Figure 3A–D), a marker of neutrophil infiltration. MPO demonstrated fewer neutrophils in the cortical region after LED treatment (P < 0.01; Figure 3B and C). Western blotting revealed that LED therapy significantly reduced MPO protein levels compared to the control group (P < 0.01; Figure 3D). We next examined microglial activation in the ischemic cortex using Iba?1 (marker protein expressed in both quiescent and active microglia) 36, 37 and CD68 (active microglia marker) 37 using immunohistochemial staining (Figure 3E–G). Iba?1/CD68 double positive cells indicated the active microglia. Iba?1(+)/CD68(+) cells in the ischemic cortex were significantly decreased in the LED therapy group relative to the control group (P < 0.05; Figure 3E and F). Morphology of Iba?1(+) microglia could be more clearly observed in Figure 3G. LED therapy remarkably reduced the Iba?1 immunoreactivies in the penumbra region of the cerebral cortex (Figure 3G). These findings suggest that neuroinflammation such as neutrophil infiltration and microglia activation after ischemic brain injury was effectively rescued by LED therapy.
Treatment with LED therapy reduced neuroinflammatory responses after ischemic stroke. (A) The coronal section illustrates the infarct region (grey) and the red rectangle indicates the imaging field. (B) LED therapy (LED?T) reduced neutrophil infiltration. Immunofluorescence staining for MPO (green), a marker for neutrophil infiltration, in control and LED?treated mouse brains 72 h after focal cerebral ischemia. (Scale bar = 100 μm). (C) Quantification graph of MPO(+) cells. (D) Western blot using ipsilateral protein showed that LED therapy decreased the expression of MPO in ischemic brain (top). The quantification graph of MPO immunoblots is shown (bottom, N = 3, ** P < 0.01 vs. control group). (E) Immunofluorescence staining for activated microglial marker Iba?1 (green) and CD68 (red) in the ischemic cortex. Fewer Iba?1(+)/CD68(+) cells (yellow) were observed in the LED therapy group. Scale bar = 100 μm. (F) Quantification graph of Iba?1(+)/CD68(+) cells. Data are expressed as the means ± SEM (N = 4). * P < 0.05 when compared with the control group (Con). (G) Iba?1 immunoreactivities were decreased in the penumbra region of the cerebral cortex with LED therapy. Magnification = ×100. The scale bar = 50 µm.
LED therapy attenuated neural cell death and inflammasome activity after ischemic brain injury
We further evaluated the effects of LED treatment on neural cell death after focal cerebral ischemia (Figures 4A and 4B). Fewer TUNEL(+)/PI(+) cells (apoptotic cells) were observed in the ischemic cortex of the LED therapy group (P < 0.05; Figure 4A and B). We next examined the effects of LED therapy on levels of inflammasome components in brain tissue ipsilateral to the lesion 72 h after ischemic insult. (Figure 4C). NLRP3 was significantly decreased in the LED therapy group relative to the control group (P < 0.05; Figure 4C). Moreover, LED therapy significantly reduced the levels of cleaved caspase?1 and ?11 (Figure 4D), as well as mature IL?1β and IL?18 in ischemic brain tissue (Figure 4E).
Post?ischemic treatment of LED therapy promoted neural cell survival in ischemic stroke through inflammasome suppression. (A) Representative photomicrographs for TUNEL (green) and PI (red). Fewer TUNEL(+)/PI(+) cells were observed in the LED therapy group (LED?T). Scale bar = 100 μm. (B) Quantification graph of TUNEL(+)/PI(+) cells in the ischemic cortex. Data are expressed as the means ± SEM (N = 4). * P < 0.05 when compared with the control group (Con). (C–E) Post?ischemic LED treatment decreases NLRP3 expression and inflammasome activity in ipsilateral side after ischemic stroke. (C) Among inflammasome component proteins such as NLRP1, NLRP3, ASC and XIAP, LED therapy decreases the level of NLRP3 (left). Quantification graph of immunoblots (right, N = 5, * P < 0.05 vs. control). (D, E) The level of activated inflammasome proteins such as cleaved?caspase?1 and cleaved?caspase?11 and maturation of IL?1β and IL?18 was investigated in ipsilateral brain tissues of C57BL/6J mice following focal cerebral ischemia. Data are expressed as the means ± SEM (N = 4 or 5). * P < 0.05, ** P < 0.01 when compared with the control group (Con).
The LED therapeutic effect on infarct reduction was mediated by NLRP3 in vivo. NLRP3 antagonist (MCC950; 10 mg/kg) or NLRP3 agonist (MSU crystals; 10 mg/kg) was administered intraperitoneally injection to mice 30 min before LED therapy. (A) After photothrombotic cortical ischemia, coronal brain sections (2 mm?thick) were stained with TTC. Blue triangle indicates the infarct area. (B) Quantification of the infarct volume was analyzed (N = 5 ∼ 7 each, means ± SEM). * P < 0.05 vs. control group (Con), ## P < 0.01, when compared with the LED?T group (one?way ANOVA). (C) LED treatment attenuates ischemic brain damage via reduction of NLRP3 level. MCC950 alone, NLRP3 inhibitor, reduced ischemic brain damage. In contrast, MSU crystal (NLRP3 agonist) blocks the LED?T effect on brain damage reduction.
We next investigated whether NLRP3 mediated the in vivo reduction of infarct volume described above (Figure 5). As seen in Figure 5, monotherapy with MCC950, a potent inhibitor of NLRP3 32 reduced infarct volume to sizes similar to LED therapy (Figure 5A and B), although the effect was not statistically significant. In contrast, an NLRP3 agonist (MSU crystals) 31 combined with LED therapy significantly inhibited the reductive effect of LED therapy effect on infarct volume (P < 0.01) (Figure 5A–C). These results indicate that post?ischemic LED therapy decreased ischemic brain damage, possibly by NLRP3?mediated inflammasome suppression.
Post?ischemic LED therapy reduced TLR?2 and triggered MAP kinase (MAPK) and NF?kB inactivation
Activation of TLRs primes NLRP3?mediated inflammasome activation, and thus cell death 38, 39, therefore, we determined expression levels of TLR?2 and TLR?4 (Figure 6A). TLR2 and TLR4 stimulation lead to priming of NLRP3 40, 41. LED therapy significantly reduced TLR?2, but not TLR?4, protein levels in the ischemic cortex (Figure 6A). We also examined MAPKs and NF?kB (Figure 6B and C) protein, as these are components of the TLR pathways. LED therapy significantly attenuated the levels of p?JNK and p?ERK, and significantly reduced translocation of the NF?κB p65 protein subunit into the nucleus, relative to the control group (P < 0.05; Figure 6B and C). These data suggest that LED therapy is capable of decreasing TLR?2?mediated signaling induced by ischemic insult.
Post?ischemic LED treatment reduced TLR?2 expression, phosphorylation of MAPKs, and NF?κB activation in a mouse ischemic stroke model. (A) TLR?2 expression in ipsilateral brain tissues was reduced in LED therapy group (LED?T). N = 5, * P < 0.05 vs. control group (Con). (B) Levels of phosphorylated p38, JNK and ERK in ipsilateral brain tissues of C57BL/6J mice following focal cerebral ischemia. LED therapy suppressed the phospho?JNK and phospho?ERK (N = 5, * P < 0.05 vs. Con). (C) Western blot analysis using ipsilateral brain tissues shows that nuclear localization of NF?kB was decreased by LED treatment. Data are expressed as the means ± SEM (N = 5, * P < 0.05 vs. Con).
Finally, we analyzed whether in vivo infarct volume reduction by LED therapy was mediated by TLR2 (Figure 7). LED therapy significantly reduced infarct volume compared to controls, but when co?treated with the TLR2 agonist Pam2CSK4 30 and LED therapy, the reduction in infarct volume was significantly inhibited (P < 0.001) (Figure 7B). These findings suggested that TLR2 mediated post?ischemic improvements by LED therapy.
Infarct volume reduction by LED therapy was mediated by TLR2 in vivo. TLR2 agonist (Pam2CSK4; 50 µg/kg) was administered intraperitoneal injection to mice 30 min before LED therapy. (A) Representative photographs of coronal brain section with TTC staining. Blue triangle indicates the infarct area. (B) Quantification of the infarct volume was analyzed (N = 5 each, means ± SEM). ** P < 0.01 vs. control group (Con), ### P < 0.001, when compared with the LED?T group (one?way ANOVA). (C) LED treatment attenuates ischemic brain damage via reduction of TLR2 level. Pam2CSK4, TLR2 agonist, blocks the LED effect.
Discussion
These studies determined that post?ischemic LED therapy reduced infarct volume in a focal cerebral ischemia mouse model. We found that LED therapy suppressed neuroinflammation and neural cell death in the ischemic cortex via TLR2?mediated activation and the NLRP3 inflammasome; and that this activation was in turn mediated through MAPK and NF?kB pathways (Figure 8). Notably, we also found improvement in neurological scores after LED therapy.
Schematic model for neuroprotection by LED therapy after ischemic stroke injury.
Interest in low?level light therapy is rapidly growing as new data on its effects are reported 21. Previous reports have demonstrated benefits including rescue of cognitive impairment and other deficits associated with chronic neurological conditions 16-20. Low?level light therapy (633 nm and 870 nm together) has improved cognition in patients with traumatic brain injury 17. Low?level light therapy also improved memory in normal adult rats 19 and middle?aged mice 42. It has been reported that near?infrared light therapy decreases depression in human subjects 16 and improves locomotor activity in rats with traumatic brain injury 18 and mice with Parkinson's disease 20. Moreover, low?level light therapy using near?infrared has reduced ischemic brain damage in experimentally induced stroke in rabbits 25, and showed neuroprotection effect in experimental stroke of rats 26, 27. It was previously reported that low?level light therapy is also effective in a pre?conditioning mode on pain, heart attack, wound healing, central nervous system and so on 43. We recently reported the preventive effect of LED therapy on ischemic brain injury of mouse 44. Since low?level light therapy is economical and has few side effects, it is applicable for clinical prevention, and not just the treatment of the cerebral ischemic disease. While the low?level light therapy mostly focused on red and near?infrared, we are interested in using low?power LED with visible light because LED using visible light are more affordable, compact/portable, and easier to use. Our results were obtained using LED therapy (610 nm orange light) applied twice a day for 3 days, commencing at 4 h after the ischemic event (Figure 2, Supplementary File), and observed the underlying mechanisms of ischemic damage reduction.
For application of light therapy, longer red/near?infrared wavelengths are much better at penetrating tissue than shorter blue/green wavelengths, therefore red and near?infrared lights are preferred clinically. There are few studies to evaluate the transmission rate of radiation in the skull 45, 46. Radiation (emitted in the 600–800 nm spectrum) can penetrate about 1 cm into the skull of human cadavers 45. Jagdeo et al. observed that 600–800 nm radiation range can penetrate soft tissues, bone, and brain parenchyma in cadavers preserved in formalin 46. Although we can suggest the penetration possibility of 610 nm light into human skull from these reports, but we don't know exactly whether our LED parameters are experimentally arrived at the target sites in human. Further investigation needed to clarify this issue.
Ischemic stroke initiates a complex cascade of pathogenetic events that lead to focal brain damage, and inflammation is a major contributor 2. Abulafia et al. 5 described a novel inflammatory mechanism through which the inflammasome contributes to neuronal cell death in cerebral ischemia 5. NLRP3 is known for its role in inflammasome formation, creating multi?protein complexes with ASC and XIAP that are critical for caspase?1 and ?11 activation, and subsequent active IL?1β/IL?18 production 10. During cerebral ischemic injury, there is increased expression of inflammasome components such as NLRP1, NLRP3, ASC, and pro?caspase?1 and ?11 5. While most innate signaling receptors have a relatively restricted ligand spectrum, NLRP3 can be activated by diverse entities such as infectious microorganisms, microbial products, dying cell fragments, and small molecule immune activators 47, 48. It has been suggested that the major role of NLRP3 inflammasomes is in
Objective: A review of photobiomodulation (PBM) in Alzheimer's dementia is submitted. The addition of PBM in neurodegenerative diseases is a dual modality that is at present gaining traction as it is safe, antiviral, and anti-inflammatory for treating neurodegeneration with photons that stimulate mitochondria increasing adenosine triphosphate and proteasomes increasing misfolded protein removal. Neurofeedback provides neural plasticity with an increase in brain-derived nerve factor mRNA and an increase in dendrite production and density in the hippocampus coupled with overall growth in dendrites, density, and neuronal survival. Background: Alzheimer's disease pathophysiology is the accumulation of hyperphosphorylated tau protein neurofibrillary tangles and subsequently amyloid-beta plaques. PBM and neurobiofeedback (NBF)address the multiple gene expression and upregulation of multiple pathogenic pathway inflammation, reactive oxidative stress, mitochondrial disorders, insulin resistance, methylation defects, regulation of neuroprotective factors, and regional hypoperfusion of the brain. There is no human evidence to suggest a clinical therapeutic benefit from using consistent light sources while significantly increasing safety concerns. Methods: A PBM test with early- to mid-Alzheimer's was reported in 2017, consisting of a double-blind, placebo-controlled trial in a small pilot group of early- to mid-dementia subjects under Institutional Review Board (IRB)-approved Food and Drug Administration (FDA) Clinical Trial. Results: PBM-treated subjects showed that active treatment subjects tended to show greater improvement in the functioning of the executive: clock drawing, immediate recall, practical memory, and visual attention and task switching (Trails A&B). A larger study using the CerebroLite helmet in Temple Texas again of subjects in a double-blind, placebo-controlled IRB-approved FDA Clinical Trial demonstrated gain in memory and cognition by increased clock drawing. Conclusions: Next-generation trials with the Cognitolite for Parkinson's disease subjects will incorporate the insights regarding significant bilateral occipital hypocoherence deficits gained from the quantitative EEG analyses. Future applications will integrate noninvasive stimulation delivery, including full-body and transcranial and infrared light with pulsed electromagnetic frequencies. Original Source: https://pubmed.ncbi.nlm.nih.gov/31647776/
Is it time to consider photobiomodulation as a drug equivalent?
Karu T. - Photomed Laser Surg. 2013 May;31(5):189-91. doi: 10.1089/pho.2013.3510. Epub 2013 Apr 19. () 865
Intro: Balance disorders, a widespread problem in the senior population, are very often related to painful musculoskeletal disabilities and/or to degenerative neurologic pathologies. In a previous work, we investigated the beneficial effects of acupuncture such as laser photobiostimulation, regardless of the etiological origin of the balance dysfunction.
Background: Balance disorders, a widespread problem in the senior population, are very often related to painful musculoskeletal disabilities and/or to degenerative neurologic pathologies. In a previous work, we investigated the beneficial effects of acupuncture such as laser photobiostimulation, regardless of the etiological origin of the balance dysfunction.
Methods: Attention was focused on two individuals showing balance deficits with different etiologies. One healthy control individual was receiving treatment, one healthy control individual did not receive any treatment. Balance performances were measured before and after ultra-low-level laser (ULLL) stimulation as a basis for the design of further investigations.
Results: Romberg's parameters were measured on a force platform. Of the four tested individuals, one showed dizziness symptoms, one was affected by a mild form of Parkinson's disease, and two showed no dysfunction and were used as controls.
Conclusions: It was found that a ULLL stimulation of peripheral Traditional Chinese Medicine (TCM) acupuncture points can be effective, regardless of the pathology.
Intro: Growing interest exists in the use of near-infrared laser therapies for the treatment of numerous neurologic conditions, including acute ischemic stroke, traumatic brain injury, Parkinson's disease, and Alzheimer's disease. In consideration of these trends, the objective of this study was to evaluate the long-term safety of transcranial laser therapy with continuous-wave (CW) near-infrared laser light (wavelength, 808 ± 10 nm, 2-mm diameter) with a nominal radiant power of 70 mW; power density, 2,230 mW/cm(2), and energy density, 268 J/cm(2) at the scalp (10 mW/cm(2) and 1.2 J/cm(2) at the cerebral cortical surface) in healthy Sprague-Dawley rats.
Background: Growing interest exists in the use of near-infrared laser therapies for the treatment of numerous neurologic conditions, including acute ischemic stroke, traumatic brain injury, Parkinson's disease, and Alzheimer's disease. In consideration of these trends, the objective of this study was to evaluate the long-term safety of transcranial laser therapy with continuous-wave (CW) near-infrared laser light (wavelength, 808 ± 10 nm, 2-mm diameter) with a nominal radiant power of 70 mW; power density, 2,230 mW/cm(2), and energy density, 268 J/cm(2) at the scalp (10 mW/cm(2) and 1.2 J/cm(2) at the cerebral cortical surface) in healthy Sprague-Dawley rats.
Abstract: Abstract
BACKGROUND AND OBJECTIVE:
Growing interest exists in the use of near-infrared laser therapies for the treatment of numerous neurologic conditions, including acute ischemic stroke, traumatic brain injury, Parkinson's disease, and Alzheimer's disease. In consideration of these trends, the objective of this study was to evaluate the long-term safety of transcranial laser therapy with continuous-wave (CW) near-infrared laser light (wavelength, 808 ± 10 nm, 2-mm diameter) with a nominal radiant power of 70 mW; power density, 2,230 mW/cm(2), and energy density, 268 J/cm(2) at the scalp (10 mW/cm(2) and 1.2 J/cm(2) at the cerebral cortical surface) in healthy Sprague-Dawley rats.
MATERIALS AND METHODS:
In this study, 120 anesthetized rats received sequential transcranial laser treatments to the right and left parietal areas of the head on the same day (minimum of 5 min between irradiation of each side), on either Day 1 or on each of Days 1, 3, and 5. Sixty anesthetized rats served as sham controls. Rats were evaluated 1 year after treatment for abnormalities in clinical hematology and brain and pituitary gland histopathology.
RESULTS:
No toxicologically important differences were found in the clinical hematology results between sham-control and laser-treated rats for any hematologic parameters examined. All values fell within historic control reference ranges for aged Sprague-Dawley rats. Similarly, brain and pituitary gland histopathology showed no treatment-related abnormalities or induced neoplasia.
CONCLUSIONS:
Single and multiple applications of transcranial laser therapy with 808-nm CW laser light at a nominal power density of 10 mW/cm(2) at the surface of the cerebral cortex appears to be safe in Sprague-Dawley rats 1 year after treatment.
Methods: In this study, 120 anesthetized rats received sequential transcranial laser treatments to the right and left parietal areas of the head on the same day (minimum of 5 min between irradiation of each side), on either Day 1 or on each of Days 1, 3, and 5. Sixty anesthetized rats served as sham controls. Rats were evaluated 1 year after treatment for abnormalities in clinical hematology and brain and pituitary gland histopathology.
Results: No toxicologically important differences were found in the clinical hematology results between sham-control and laser-treated rats for any hematologic parameters examined. All values fell within historic control reference ranges for aged Sprague-Dawley rats. Similarly, brain and pituitary gland histopathology showed no treatment-related abnormalities or induced neoplasia.
Conclusions: Single and multiple applications of transcranial laser therapy with 808-nm CW laser light at a nominal power density of 10 mW/cm(2) at the surface of the cerebral cortex appears to be safe in Sprague-Dawley rats 1 year after treatment.
Intro: It has been hypothesized that reduced axonal transport contributes to the degeneration of neuronal processes in Parkinson's disease (PD). Mitochondria supply the adenosine triphosphate (ATP) needed to support axonal transport and contribute to many other cellular functions essential for the survival of neuronal cells. Furthermore, mitochondria in PD tissues are metabolically and functionally compromised. To address this hypothesis, we measured the velocity of mitochondrial movement in human transmitochondrial cybrid "cytoplasmic hybrid" neuronal cells bearing mitochondrial DNA from patients with sporadic PD and disease-free age-matched volunteer controls (CNT). The absorption of low level, near-infrared laser light by components of the mitochondrial electron transport chain (mtETC) enhances mitochondrial metabolism, stimulates oxidative phosphorylation and improves redox capacity. PD and CNT cybrid neuronal cells were exposed to near-infrared laser light to determine if the velocity of mitochondrial movement can be restored by low level light therapy (LLLT). Axonal transport of labeled mitochondria was documented by time lapse microscopy in dopaminergic PD and CNT cybrid neuronal cells before and after illumination with an 810 nm diode laser (50 mW/cm2) for 40 seconds. Oxygen utilization and assembly of mtETC complexes were also determined.
Background: It has been hypothesized that reduced axonal transport contributes to the degeneration of neuronal processes in Parkinson's disease (PD). Mitochondria supply the adenosine triphosphate (ATP) needed to support axonal transport and contribute to many other cellular functions essential for the survival of neuronal cells. Furthermore, mitochondria in PD tissues are metabolically and functionally compromised. To address this hypothesis, we measured the velocity of mitochondrial movement in human transmitochondrial cybrid "cytoplasmic hybrid" neuronal cells bearing mitochondrial DNA from patients with sporadic PD and disease-free age-matched volunteer controls (CNT). The absorption of low level, near-infrared laser light by components of the mitochondrial electron transport chain (mtETC) enhances mitochondrial metabolism, stimulates oxidative phosphorylation and improves redox capacity. PD and CNT cybrid neuronal cells were exposed to near-infrared laser light to determine if the velocity of mitochondrial movement can be restored by low level light therapy (LLLT). Axonal transport of labeled mitochondria was documented by time lapse microscopy in dopaminergic PD and CNT cybrid neuronal cells before and after illumination with an 810 nm diode laser (50 mW/cm2) for 40 seconds. Oxygen utilization and assembly of mtETC complexes were also determined.
Abstract: Abstract
BACKGROUND:
It has been hypothesized that reduced axonal transport contributes to the degeneration of neuronal processes in Parkinson's disease (PD). Mitochondria supply the adenosine triphosphate (ATP) needed to support axonal transport and contribute to many other cellular functions essential for the survival of neuronal cells. Furthermore, mitochondria in PD tissues are metabolically and functionally compromised. To address this hypothesis, we measured the velocity of mitochondrial movement in human transmitochondrial cybrid "cytoplasmic hybrid" neuronal cells bearing mitochondrial DNA from patients with sporadic PD and disease-free age-matched volunteer controls (CNT). The absorption of low level, near-infrared laser light by components of the mitochondrial electron transport chain (mtETC) enhances mitochondrial metabolism, stimulates oxidative phosphorylation and improves redox capacity. PD and CNT cybrid neuronal cells were exposed to near-infrared laser light to determine if the velocity of mitochondrial movement can be restored by low level light therapy (LLLT). Axonal transport of labeled mitochondria was documented by time lapse microscopy in dopaminergic PD and CNT cybrid neuronal cells before and after illumination with an 810 nm diode laser (50 mW/cm2) for 40 seconds. Oxygen utilization and assembly of mtETC complexes were also determined.
RESULTS:
The velocity of mitochondrial movement in PD cybrid neuronal cells (0.175 +/- 0.005 SEM) was significantly reduced (p < 0.02) compared to mitochondrial movement in disease free CNT cybrid neuronal cells (0.232 +/- 0.017 SEM). For two hours after LLLT, the average velocity of mitochondrial movement in PD cybrid neurites was significantly (p < 0.003) increased (to 0.224 +/- 0.02 SEM) and restored to levels comparable to CNT. Mitochondrial movement in CNT cybrid neurites was unaltered by LLLT (0.232 +/- 0.017 SEM). Assembly of complexes in the mtETC was reduced and oxygen utilization was altered in PD cybrid neuronal cells. PD cybrid neuronal cell lines with the most dysfunctional mtETC assembly and oxygen utilization profiles were least responsive to LLLT.
CONCLUSION:
The results from this study support our proposal that axonal transport is reduced in sporadic PD and that a single, brief treatment with near-infrared light can restore axonal transport to control levels. These results are the first demonstration that LLLT can increase axonal transport in model human dopaminergic neuronal cells and they suggest that LLLT could be developed as a novel treatment to improve neuronal function in patients with PD.
Methods: The velocity of mitochondrial movement in PD cybrid neuronal cells (0.175 +/- 0.005 SEM) was significantly reduced (p < 0.02) compared to mitochondrial movement in disease free CNT cybrid neuronal cells (0.232 +/- 0.017 SEM). For two hours after LLLT, the average velocity of mitochondrial movement in PD cybrid neurites was significantly (p < 0.003) increased (to 0.224 +/- 0.02 SEM) and restored to levels comparable to CNT. Mitochondrial movement in CNT cybrid neurites was unaltered by LLLT (0.232 +/- 0.017 SEM). Assembly of complexes in the mtETC was reduced and oxygen utilization was altered in PD cybrid neuronal cells. PD cybrid neuronal cell lines with the most dysfunctional mtETC assembly and oxygen utilization profiles were least responsive to LLLT.
Results: The results from this study support our proposal that axonal transport is reduced in sporadic PD and that a single, brief treatment with near-infrared light can restore axonal transport to control levels. These results are the first demonstration that LLLT can increase axonal transport in model human dopaminergic neuronal cells and they suggest that LLLT could be developed as a novel treatment to improve neuronal function in patients with PD.
Intro: The influence of laser therapy on the course of Parkinson's disease (PD) was studied in 70 patients. This influence appeared adaptogenic both in the group with elevated and low MAO B and Cu/Zn SOD activity. Laser therapy resulted in reduction of neurological deficit, normalization of the activity of MAO B, Cu/Zn-SOD and immune indices. There was a correlation between humoral immunity and activity of the antioxidant enzymes (SOD, catalase). This justifies pathogenetically the use of laser therapy in PD.
Background: The influence of laser therapy on the course of Parkinson's disease (PD) was studied in 70 patients. This influence appeared adaptogenic both in the group with elevated and low MAO B and Cu/Zn SOD activity. Laser therapy resulted in reduction of neurological deficit, normalization of the activity of MAO B, Cu/Zn-SOD and immune indices. There was a correlation between humoral immunity and activity of the antioxidant enzymes (SOD, catalase). This justifies pathogenetically the use of laser therapy in PD.
Abstract: Abstract
The influence of laser therapy on the course of Parkinson's disease (PD) was studied in 70 patients. This influence appeared adaptogenic both in the group with elevated and low MAO B and Cu/Zn SOD activity. Laser therapy resulted in reduction of neurological deficit, normalization of the activity of MAO B, Cu/Zn-SOD and immune indices. There was a correlation between humoral immunity and activity of the antioxidant enzymes (SOD, catalase). This justifies pathogenetically the use of laser therapy in PD.
Laboratory of Molecular and Chemical Biology of Neurodegeneration, Brain Mind Institute, Swiss Federal Institute of Technology (EPFL), CH-1015, Lausanne, Switzerland; Centre de Recherche du Centre Hospitalier de Quebec, Axe Neuroscience et Departement de Medecine Moleculaire de l'Universite Laval, Quebec, G1V4G2, Canada. Institute of Chemical Sciences and Engineering, Swiss Federal Institute of Technology (EPFL), CH-1015, Lausanne, Switzerland; Medos International Sarl, a Johnson&Johnson company, Chemin Blanc 38, CH-2400, Le Locle, Switzerland. Medos International Sarl. Qatar Biomedical Research Institute, Hamad Bin Khalifa University, Qatar Foundation, P.O. Box 5825, Doha, Qatar.
Converging lines of evidence indicate that near-infrared light treatment, also known as photobiomodulation (PBM), may exert beneficial effects and protect against cellular toxicity and degeneration in several animal models of human pathologies, including neurodegenerative disorders. In the present study, we report that chronic PMB treatment mitigates dopaminergic loss induced by unilateral overexpression of human alpha-synuclein (alpha-syn) in the substantia nigra of an AAV-based rat genetic model of Parkinson's disease (PD). In this model, daily exposure of both sides of the rat's head to 808-nm near-infrared light for 28 consecutive days alleviated alpha-syn-induced motor impairment, as assessed using the cylinder test. This treatment also significantly reduced dopaminergic neuronal loss in the injected substantia nigra and preserved dopaminergic fibers in the ipsilateral striatum. These beneficial effects were sustained for at least 6 weeks after discontinuing the treatment. Together, our data point to PBM as a possible therapeutic strategy for the treatment of PD and other related synucleinopathies.
Laboratory of Molecular and Chemical Biology of Neurodegeneration, Brain Mind Institute, Swiss Federal Institute of Technology (EPFL), CH-1015, Lausanne, Switzerland; Centre de Recherche du Centre Hospitalier de Quebec, Axe Neuroscience et Departement de Medecine Moleculaire de l'Universite Laval, Quebec, G1V4G2, Canada. Institute of Chemical Sciences and Engineering, Swiss Federal Institute of Technology (EPFL), CH-1015, Lausanne, Switzerland; Medos International Sarl, a Johnson&Johnson company, Chemin Blanc 38, CH-2400, Le Locle, Switzerland. Medos International Sarl. Qatar Biomedical Research Institute, Hamad Bin Khalifa University, Qatar Foundation, P.O. Box 5825, Doha, Qatar.
Converging lines of evidence indicate that near-infrared light treatment, also known as photobiomodulation (PBM), may exert beneficial effects and protect against cellular toxicity and degeneration in several animal models of human pathologies, including neurodegenerative disorders. In the present study, we report that chronic PMB treatment mitigates dopaminergic loss induced by unilateral overexpression of human alpha-synuclein (alpha-syn) in the substantia nigra of an AAV-based rat genetic model of Parkinson's disease (PD). In this model, daily exposure of both sides of the rat's head to 808-nm near-infrared light for 28 consecutive days alleviated alpha-syn-induced motor impairment, as assessed using the cylinder test. This treatment also significantly reduced dopaminergic neuronal loss in the injected substantia nigra and preserved dopaminergic fibers in the ipsilateral striatum. These beneficial effects were sustained for at least 6 weeks after discontinuing the treatment. Together, our data point to PBM as a possible therapeutic strategy for the treatment of PD and other related synucleinopathies.
Federal Institute of Technology (EPFL), Institute of Chemical Sciences and Engineering (ISIC), 1015 Lausanne, Switzerland.
Photobiomodulation (PBM) appears promising to treat the hallmarks of Parkinson's Disease (PD) in cellular or animal models. We measured light propagation in different areas of PD-relevant deep brain tissue during transcranial, transsphenoidal illumination (at 671 and 808 nm) of a cadaver head and modeled optical parameters of human brain tissue using Monte-Carlo simulations. Gray matter, white matter, cerebrospinal fluid, ventricles, thalamus, pons, cerebellum and skull bone were processed into a mesh of the skull (158 x 201 x 211 voxels; voxel side length: 1 mm). Optical parameters were optimized from simulated and measured fluence rate distributions. The estimated mueff for the different tissues was in all cases larger at 671 than at 808 nm, making latter a better choice for light delivery in the deep brain. Absolute values were comparable to those found in the literature or slightly smaller. The effective attenuation in the ventricles was considerably larger than literature values. Optimization yields a new set of optical parameters better reproducing the experimental data. A combination of PBM via the sphenoid sinus and oral cavity could be beneficial. A 20-fold higher efficiency of light delivery to the deep brain was achieved with ventricular instead of transcranial illumination. Our study demonstrates that it is possible to illuminate deep brain tissues transcranially, transsphenoidally and via different application routes. This opens therapeutic options for sufferers of PD or other cerebral diseases necessitating light therapy.
Laser Acupuncture at HT7 Acupoint Improves Cognitive Deficit, Neuronal Loss, Oxidative Stress, and Functions of Cholinergic and Dopaminergic Systems in Animal Model of Parkinson's Disease.
Department of Physiology, Faculty of Medicine, Khon Kaen University, Khon Kaen 40002, Thailand ; Integrative Complementary Alternative Medicine Research and Development Center, Khon Kaen University, Khon Kaen 40002, Thailand. Integrative Complementary Alternative Medicine Research and Development Center, Khon Kaen University, Khon Kaen 40002, Thailand ; Department of Physiology, Neuroscience Program, Faculty of Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
To date, the therapeutic strategy against cognitive impairment in Parkinson's disease (PD) is still not in satisfaction level and requires novel effective intervention. Based the oxidative stress reduction and cognitive enhancement induced by laser acupuncture at HT7, the beneficial effect of laser acupuncture at HT7 against cognitive impairment in PD has been focused. In this study, we aimed to determine the effect of laser acupuncture at HT7 on memory impairment, oxidative stress status, and the functions of both cholinergic and dopaminergic systems in hippocampus of animal model of PD. Male Wistar rats, weighing 180-220 g, were induced unilateral lesion at right substantianigra by 6-OHDA and were treated with laser acupuncture continuously at a period of 14 days. The results showed that laser acupuncture at HT7 enhanced memory and neuron density in CA3 and dentate gyrus. The decreased AChE, MAO-B, and MDA together with increased GSH-Px in hippocampus of a 6-OHDA lesion rats were also observed. In conclusion, laser acupuncture at HT7 can improve neuron degeneration and memory impairment in animal model of PD partly via the decreased oxidative stress and the improved cholinergic and dopaminergic functions. More researches concerning effect of treatment duration are still required.
Photobiomodulation with near infrared light mitigates Alzheimer's disease- related pathology in cerebral cortex - evidence from two transgenic mouse models.
Bosch Institute, University of Sydney NSW 2006, Australia. Daniel.Johnstone@sydney.edu.au
INTRODUCTION: Previous work has demonstrated the efficacy of irradiating tissue with red to infrared light in mitigating cerebral pathology and degeneration in animal models of stroke, traumatic brain injury, parkinsonism and Alzheimer's disease (AD). Using mouse models, we explored the neuroprotective effect of near infrared light (NIr) treatment, delivered at an age when substantial pathology is already present in the cerebral cortex.
METHODS: We studied two mouse models with AD- related pathologies: the K369I tau transgenic model (K3), engineered to develop neurofibrillary tangles, and the APPswe/PSEN1dE9 transgenic model (APP/PS1), engineered to develop amyloid plaques. Mice were treated with NIr 20 times over a four-week period and histochemistry was used to quantify AD- related pathological hallmarks and other markers of cell damage in the neocortex and hippocampus.
RESULTS: In the K3 mice, NIr treatment was associated with a reduction in hyperphosphorylated tau, neurofibrillary tangles and oxidative stress markers (4-hydroxynonenal and 8-hydroxy-2'- deoxyguanosine) to near wildtype levels in the neocortex and hippocampus, and with a restoration of expression of the mitochondrial marker cytochrome c oxidase in surviving neurons. In the APP/PS1 mice, NIr treatment was associated with a reduction in the size and number of amyloid-beta plaques in the neocortex and hippocampus.
CONCLUSIONS: Our results, in two transgenic mouse models, suggest that NIr may have potential as an effective, minimally-invasive intervention for mitigating, and even reversing, progressive cerebral degenerations.
Photobiomodulation inside the brain: a novel method of applying near- infrared light intracranially and its impact on dopaminergic cell survival in MPTP-treated mice.
Moro C, Massri NE, Torres N, Ratel D, De Jaeger X, Chabrol C, Perraut F, Bourgerette A, Berger M, Purushothuman S, Johnstone D, Stone J, Mitrofanis J, Benabid AL CEA-Leti, Grenoble, France; - (Publication) 4432
Object Previous experimental studies have documented the neuroprotection of damaged or diseased cells after applying, from outside the brain, near-infrared light (NIr) to the brain by using external light- emitting diodes (LEDs) or laser devices. In the present study, the authors describe an effective and reliable surgical method of applying to the brain, from inside the brain, NIr to the brain. They developed a novel internal surgical device that delivers the NIr to brain regions very close to target damaged or diseased cells. They suggest that this device will be useful in applying NIr within the large human brain, particularly if the target cells have a very deep location. Methods An optical fiber linked to an LED or laser device was surgically implanted into the lateral ventricle of BALB/c mice or Sprague-Dawley rats.
The authors explored the feasibility of the internal device, measured the NIr signal through living tissue, looked for evidence of toxicity at doses higher than those required for neuroprotection, and confirmed the neuroprotective effect of NIr on dopaminergic cells in the substantia nigra pars compacta (SNc) in an acute 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) model of Parkinson disease in mice. Results The device was stable in freely moving animals, and the NIr filled the cranial cavity. Measurements showed that the NIr intensity declined as distance from the source increased across the brain (65% per mm) but was detectable up to 10 mm away. At neuroprotective (0.16 mW) and much higher (67 mW) intensities, the NIr caused no observable behavioral deficits, nor was there evidence of tissue necrosis at the fiber tip, where radiation was most intense. Finally, the intracranially delivered NIr protected SNc cells against MPTP insult; there were consistently more dopaminergic cells in MPTP-treated mice irradiated with NIr than in those that were not irradiated. Conclusions In summary, the authors showed that NIr can be applied intracranially, does not have toxic side effects, and is neuroprotective.
We have shown previously that photobiomodulation or near-infrared light (NIr) treatment protects dopaminergic cells of the substantia nigra pars compacta (SNc) in an acute MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) model of Parkinson's disease (PD). In this study, we tested the protective and rescue action of NIr treatment in a chronic MPTP model, developed to resemble more closely the slow progressive degeneration in PD patients. We examined three regions of dopaminergic cells, the SNc, periaqueductal grey matter (PaG) and zona incerta-hypothalamus (ZI-Hyp). BALB/c mice had MPTP or saline injections over five weeks, followed by a three-week survival. NIr treatment was applied either at the same time as (simultaneous series) or after (post-treatment series) the MPTP insult. There were four groups within each series; Saline, Saline-NIr, MPTP and MPTP-NIr. Brains were processed for tyrosine hydroxylase (TH) immunochemistry and cell number was analysed using the optical fractionator method. In the SNc, there was a significant reduction ( approximately 45%) in TH(+) cell number in the MPTP groups compared to the saline controls of both series. In the MPTP-NIr groups of both series, TH(+) cell number was significantly higher ( approximately 25%) than in the MPTP groups, but lower than in the saline controls ( approximately 20%). By contrast in the PaG and ZI-Hyp, there were no significant differences in TH(+) cell number between the MPTP an MPTP-NIr groups of either series. In summary, exposure to NIr either at the same time or well after chronic MPTP insult saved many SNc dopaminergic cells from degeneration.
Department of Neurology, Medical College of Wisconsin, 8701 W. Watertown Plank Rd, Milwaukee, WI, 53226, USA.
Parkinson's disease (PD) is a neurodegenerative disorder that affects large numbers of people, particularly those of a more advanced age. Mitochondrial dysfunction plays a central role in PD, especially in the electron transport chain. This mitochondrial role allows the use of inhibitors of complex I and IV in PD models, and enhancers of complex IV activity, such as NIR light, to be used as possible therapy. PD models fall into two main categories; cell cultures and animal models. In cell cultures, primary neurons, mutant neuroblastoma cells, and cell cybrids have been studied in conjunction with NIR light. Primary neurons show protection or recovery of function and morphology by NIR light after toxic insult.
Neuroblastoma cells, with a gene for mutant alpha-synuclein, show similar results. Cell cybrids, containing mtDNA from PD patients, show restoration of mitochondrial transport and complex I and IV assembly. Animal models include toxin-insulted mice, and alpha-synuclein transgenic mice. Functional recovery of the animals, chemical and histological evidence, and delayed disease progression show the potential of NIR light in treating Parkinson's disease.
University of Virginia, Morris K Udall Parkinson's Research Center of Excellence and Department of Neurology, Charlottesville, Virginia, USA. pat5q@virginia.edu.
ABSTRACT: BACKGROUND: It has been hypothesized that reduced axonal transport contributes to the degeneration of neuronal processes in Parkinson's disease (PD). Mitochondria supply the adenosine triphosphate (ATP) needed to support axonal transport and contribute to many other cellular functions essential for the survival of neuronal cells. Furthermore, mitochondria in PD tissues are metabolically and functionally compromised. To address this hypothesis, we measured the velocity of mitochondrial movement in human transmitochondrial cybrid "cytoplasmic hybrid" neuronal cells bearing mitochondrial DNA from patients with sporadic PD and disease-free age-matched volunteer controls (CNT). The absorption of low level, near-infrared laser light by components of the mitochondrial electron transport chain (mtETC) enhances mitochondrial metabolism, stimulates oxidative phosphorylation and improves redox capacity. PD and CNT cybrid neuronal cells were exposed to near-infrared laser light to determine if the velocity of mitochondrial movement can be restored by low level light therapy (LLLT).
Axonal transport of labeled mitochondria was documented by time lapse microscopy in dopaminergic PD and CNT cybrid neuronal cells before and after illumination with an 810 nm diode laser (50 mW/cm2) for 40 seconds. Oxygen utilization and assembly of mtETC complexes were also determined.
RESULTS: The velocity of mitochondrial movement in PD cybrid neuronal cells (0.175 +/- 0.005 SEM) was significantly reduced (p < 0.02) compared to mitochondrial movement in disease free CNT cybrid neuronal cells (0.232 +/- 0.017 SEM). For two hours after LLLT, the average velocity of mitochondrial movement in PD cybrid neurites was significantly (p < 0.003) increased (to 0.224 +/- 0.02 SEM) and restored to levels comparable to CNT. Mitochondrial movement in CNT cybrid neurites was unaltered by LLLT (0.232 +/- 0.017 SEM). Assembly of complexes in the mtETC was reduced and oxygen utilization was altered in PD cybrid neuronal cells. PD cybrid neuronal cell lines with the most dysfunctional mtETC assembly and oxygen utilization profiles were least responsive to LLLT.
CONCLUSION: The results from this study support our proposal that axonal transport is reduced in sporadic PD and that a single, brief treatment with near-infrared light can restore axonal transport to control levels. These results are the first demonstration that LLLT can increase axonal transport in model human dopaminergic neuronal cells and they suggest that LLLT could be developed as a novel treatment to improve neuronal function in patients with PD.
Morris K. Udall Parkinson's Disease Research Center of Excellence, Department of Neurology, University of Virginia, Charlottesville, VA 22908, USA.
Parkinson's disease (PD) is the eponym attached to the most prevalent neurodegenerative movement disorder of adults, derived from observations of an early nineteenth century physician and paleontologist, James Parkinson, and is now recognized to encompass much more than a movement disorder clinically or dopamine neuron death pathologically. Most PD ( approximately 90%) is sporadic (sPD), is associated with mitochondrial deficiencies and has been studied in cell and animal models arising from the use of mitochondrial toxins that unfortunately have not predicted clinical efficacy to slow disease progression in humans. We have extensively studied the cytoplasmic hybrid ("cybrid") model of sPD in which donor mtDNAs are introduced into and expressed in neural tumor cells with identical nuclear genetic and environmental backgrounds. sPD cybrids demonstrate many abnormalities in which increased oxidative stress drives downstream antioxidant response and cell death activating signaling pathways. sPD cybrids regulate mitochondrial ETC genes and gene ontology families like sPD brain. sPD cybrids spontaneously form Lewy bodies and Lewy neurites, linking mtDNA expression to neuropathology, and demonstrate impaired organelle transport in processes and reduced mitochondrial respiration. Our recent studies show that near-infrared laser light therapy normalizes mitochondrial movement and can stimulate respiration in sPD cybrid neurons, and mitochondrial gene therapy can restore respiration and stimulate mitochondrial ETC gene and protein expression. sPD cybrids have provided multiple lines of circumstantial evidence linking mtDNA to sPD pathogenesis and can serve as platforms for therapy development. sPD cybrid models can be improved by the use of non-tumor human stem cell-derived neural precursor cells and by an introduction of postmortem brain mtDNA to test its causality directly.
This tool is a searchable collection of technical publications, books, videos and other resources about the use of lasers and light for PhotoBioModulation (PBM). Enter a keyword above or see some of our favorite queries below.
All the resources include links to the original source so we are not making any statement about the use of lasers for treating non-FDA cleared application, we are simple summarizing what others have said.
Where every possible, we have included a link to the orginal publication.
This tool uses a broad match query so:
It does not correct spelling and searches only cold laser related subjects so do not use LLLT, cold or laser in the search bar
It works better with shorter search terms or even parts of search terms
It searches all the available fields so you can enter a body part, author, condition or laser brand.
Where ever possible, the detailed section about the resource will link to the sources.
This system is only for photobiomodulation or cold laser therapy research (including LLLT, laser acupuncture and high power laser therapy) only. It does NOT include photodynamic laser therapy (where the laser is used to react with a pharmaceutical), hot surgery lasers or cosmetic lasers. It does include some resources on weight loss and smoking cessation.
The results of the search are sorted based on 3 quality factors on a scale of 1 to 10 with 10 being the best score. Originally all the resources were given a 5-5-5 until they could be individually evaluated. These scores are purely opinion and are only used to simplify the rank of the results from more valuable to least valuable. This should not be considered a critique of any work. This system was created to help researchers (including ourselves) find the most usable resources for any cold laser therapy research. The resources are assigned values based on the following 3 factors:
Efficacy: The resource (especially research papers) should show a significant improvement in the condition being treated. Resources that show better results are given a higher quality score.
Detail: The source must give enough information that the results can be duplicated. If a resource lacks too many details that it cannot be recreated, it is given a lower detail score.
Lack of Bias: Many resources are created to try and show that one device is superior to its competition. Many manufacturers have staff that crank out biased papers on a regular basis on the hope that this will make their product look superior. If the author of the resource is paid by a manufacturer of the resource appears to be biased towards one device and not one technology, the resource has much less value.
Over the past few years of working with research, we found that a majority of the published resources are lacking in one of these three ranking factors.
The original goal of this research tool was to tie published resources to the protocols in the laser-therapy.us library. This connection allows users to trace each protocol back to a list of resources so the protocol can be researched and improved.
General Comments
POWER
When many of the first research papers were published, the most power laser available for therapy were less than 100mW and many systems had to be pulsed to keep the laser from burning out too quickly. Today, system are available that will deliver up to 60,000mW of continuous output. Because of these power limitation, many early studies were limited to extremely low dosages by today’s standards. It takes a 50mW system 17 minutes to deliver 50 joules at the surface of the skin. If this was spread over a large area of damage or was treating a deeper problem, the actual dosages were much less than 1J/cm2. Today, we know that these dosages typically produce very little or no results. WAVELENGTH
About 80% of the resources in this database are in the near infrared wavelength. There is also some interest in the red wavelength (600 to 660nm) . Other wavelengths like blue, purple, and green have very little scientific research behind them and have not gotten much traction in the core therapy market with the exception of some fringe consumer products. Legal Disclaimer This research tool is free to use but we make no claims about the accuracy of the information. It is an aggregation of existing published resources and it is up to the user to determine if the source of the resources has any value. The information provided through this web site should not be used for diagnosing or treating a health problem or disease. If you have or suspect you may have a health problem, you should consult your local health care provider.
Welcome to the BioPhotonica Education Center. There are over 5000 successful studies showing the efficacy of PBM, light therapy and sound therapy. This is a searchable collection of technical publications, books, videos and other resources about the best practices in the industry and about treating a wide variety of problems. All the resources include links to the original source (where available) so we are not making any claims about the use of our technology for treating "non-FDA cleared" applications, we are simply summarizing what the expert are saying about proper application of these technologies.
Enter a keyword above and click on one of the following links to see a set of publications about that subject. HINT: Shorter keywords work better.
It does not correct spelling and searches only PBM related subjects so do not use LLLT, cold or laser in the search bar
It works better with shorter search terms or even parts of search terms
It searches all the available fields so you can enter a body part, author, condition or laser brand.
This system is only for photobiomodulation or cold laser therapy research (including LLLT, laser acupuncture and high power laser therapy) only. It does NOT include photodynamic laser therapy (where the laser is used to react with a pharmaceutical), hot surgery lasers or cosmetic therapies.
Welcome to the Lighthouse Health Education Center. There are over 5000 successful studies showing the efficacy of PBM, light therapy and sound therapy. This is a searchable collection of technical publications, books, videos and other resources about the best practices in the industry and about treating a wide variety of problems. All the resources include links to the original source (where available) so we are not making any claims about the use of our technology for treating "non-FDA cleared" applications, we are simply summarizing what the expert are saying about proper application of these technologies.
Enter a keyword above and click on one of the following links to see a set of publications about that subject. HINT: Shorter keywords work better.
It does not correct spelling and searches only cold laser related subjects so do not use LLLT, cold or laser in the search bar
It works better with shorter search terms or even parts of search terms
It searches all the available fields so you can enter a body part, author, condition or laser brand.
This system is only for photobiomodulation or cold laser therapy research (including LLLT, laser acupuncture and high power laser therapy) only. It does NOT include photodynamic laser therapy (where the laser is used to react with a pharmaceutical), hot surgery lasers or cosmetic therapies.
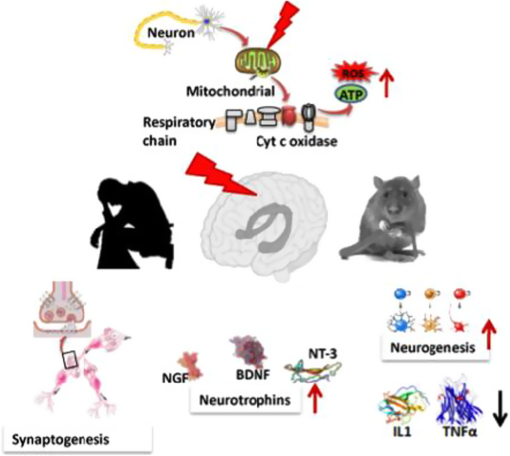




















 Diagram of the various medical applications of low-level light therapy.
Diagram of the various medical applications of low-level light therapy.
 Illustration of mitochondrion, as well as of the electron transport chain and oxidative metabolism.
Illustration of mitochondrion, as well as of the electron transport chain and oxidative metabolism.
 Complex IV (cytochrome c oxidase) is the principal chromophore involved in low-level light therapy. It has 2 copper centers and 2 heme prosthetic groups. Cytochrome c is oxidized and oxygen is reduced to water during respiration.
Complex IV (cytochrome c oxidase) is the principal chromophore involved in low-level light therapy. It has 2 copper centers and 2 heme prosthetic groups. Cytochrome c is oxidized and oxygen is reduced to water during respiration.
 Nitric oxide can bind to copper (or heme) centers in cytochrome c oxidase and inhibit respiration. The nitric oxide may be photodissociated by absorption of red or near infrared light, allowing oxygen to return and sharply increasing respiration and adenosine ...
Nitric oxide can bind to copper (or heme) centers in cytochrome c oxidase and inhibit respiration. The nitric oxide may be photodissociated by absorption of red or near infrared light, allowing oxygen to return and sharply increasing respiration and adenosine ...
 Diagram that illustrates the mechanism of low-level light therapy (LLLT) on the cellular and molecular level. Near infrared light, absorbed by the mitochondria, causes upregulation of the cellular respiratory chain. A host of downstream cellular responses ...
Diagram that illustrates the mechanism of low-level light therapy (LLLT) on the cellular and molecular level. Near infrared light, absorbed by the mitochondria, causes upregulation of the cellular respiratory chain. A host of downstream cellular responses ...
 Location of periventricular white matter (PVWM) area (black arrow), adjacent to the body of the lateral ventricle, located immediately superior to the posterior limb, internal capsule (computed tomography slice angulation, coronal and axial views). An ...
Location of periventricular white matter (PVWM) area (black arrow), adjacent to the body of the lateral ventricle, located immediately superior to the posterior limb, internal capsule (computed tomography slice angulation, coronal and axial views). An ...
 (a.) Computed tomography (CT) scan of a 65-year-old woman obtained 5 months after stroke onset shows sparing of the most posterior portion of the periventricular white matter (PVWM) (white arrow), that is, likely sparing of some of the leg fibers. This ...
(a.) Computed tomography (CT) scan of a 65-year-old woman obtained 5 months after stroke onset shows sparing of the most posterior portion of the periventricular white matter (PVWM) (white arrow), that is, likely sparing of some of the leg fibers. This ...
 (a.) Before the first low-level laser therapy (LLLT) and microamps transcutaneous electrical nerve stimulation (TENS) acupuncture treatment. It was 1.5 years after stroke onset and the patient still had right hand spasticity and was unable to extend her ...
(a.) Before the first low-level laser therapy (LLLT) and microamps transcutaneous electrical nerve stimulation (TENS) acupuncture treatment. It was 1.5 years after stroke onset and the patient still had right hand spasticity and was unable to extend her ...
 (a.) Red and near-infrared (NIR) light-emitting diode (LED) cluster head (2-inch diameter) for transcranial LED treatments. (b.) Sample placement location on right forehead for one of the LED cluster heads during transcranial LED treatment. (c.) Graph ...
(a.) Red and near-infrared (NIR) light-emitting diode (LED) cluster head (2-inch diameter) for transcranial LED treatments. (b.) Sample placement location on right forehead for one of the LED cluster heads during transcranial LED treatment. (c.) Graph ...